Older posts on the virus/disease
(Facebook)
Comment on this (at bottom of page)
March 1st, 2020:
You didn't ask, but here goes.
I believe that the number of people currently infected with the coronavirus in the US is somewhere around 15,000.
This is based on the current infection rates in both South Korea (0.007% of total population) and Italy (0.002% of total population)
Both of those countries have engaged in aggressive testing of their populations. South Korea by actually testing (they have tested over 110,000 people) and Italy by setting the diagnosis criteria as clinical presentation (i.e. if you show up with a fever, coughing, sneezing, pneumonia -- they assume it's coronavirus without actually testing for it)
The US, by contrast, has chosen a "see no evil" approach and is actively denying that the virus is here by simply not looking for it (i.e. testing)
Absent large-scale measures to limit transmission (such as school closing, mandatory telework, internal travel bans, etc.) it is likely that 40-60% of the US population will eventually contract "the coronavirus." That's 160 million people.
That's the bad news. The good news is that of those 160 million, 90% or ~145 million will have little to no symptoms at all.
The bad news is that 15 million people will have serious symptoms and require intensive medical care. Of those 15 million, 5 million will die.
The good news is that there are 4 million doctors and nurses in this country. And another 7-10 million people with sufficient training to act as effective proxies for the licensed caregivers I mentioned above. I.e. people who can evaluate cases, triage and administer medication and other palliative measures.
Good news: That's a nearly 1:1 match with those that need medical attention, in a worst-case scenario. Now of course not all will be available, so let's call it a 1:0.5 match.
Bad news is that there are nowhere near enough hospital beds in the US for the 15 million that need them (there are about 800,000 beds today in the US, down from 1.5 million in 1975, the result of the rise of "regional" medical centers and the closing of rural hospitals as a result)
Good news is, even if we did have the beds, hospitals are no places for the sick.
What we should do, I believe, is instigate at the federal level a massive program to facilitate self-quarantine and other effective prophylactic measures. Those include:
1. Federal job protections for anyone who self-quarantines. Meaning you cannot be fired or suffer punishment for job absences of up to a month when justified on a quarantine basis.
2. Very large no-interest loans and/or substantial tax advantages to any company which continues to pay its workers who self quarantine. This includes hourly minimum-wage workers on up.
3. Widespread closures of schools from kindergarten through graduate education. Again, with federal financial support to those institutions which voluntarily close
4. The mobilization of a traveling medical corps from the pool of individuals I mentioned above. This should come under military jurisdiction because of the logistical factors. Basically a wholesale mobilization of medical caregivers under military command. They would be transported on a case basis to those who are at-risk (the 10%) and require medical care. Think an armada of olive-drab schoolhouses (we can use some of the buses idled when the schools are closed) taking medical personnel door-to-door on a daily basis.
Numbers-wise each medical professional will visit two critical patients per day, every day. In their homes or other facilities where needed (i.e. skilled nursing facilities)
5. The rapid creation of a large-scale manufacturing base capable of turning out antibiotics and other palliative medication as well as necessary medical equipment (syringes, saline solution, drip bags, thermometers, etc.). The country is full of disused and/or abandoned factories that should be mobilized towards this effort.
6. Finally, a wide-scale public education program on how to limit transmission. Starts with no touching anyone. Washing your hands. Internal travel bans. Avoid congregation (church, sporting events, conferences, etc.)
You didn't ask, but here goes.
I believe that the number of people currently infected with the coronavirus in the US is somewhere around 15,000.
This is based on the current infection rates in both South Korea (0.007% of total population) and Italy (0.002% of total population)
Both of those countries have engaged in aggressive testing of their populations. South Korea by actually testing (they have tested over 110,000 people) and Italy by setting the diagnosis criteria as clinical presentation (i.e. if you show up with a fever, coughing, sneezing, pneumonia -- they assume it's coronavirus without actually testing for it)
The US, by contrast, has chosen a "see no evil" approach and is actively denying that the virus is here by simply not looking for it (i.e. testing)
Absent large-scale measures to limit transmission (such as school closing, mandatory telework, internal travel bans, etc.) it is likely that 40-60% of the US population will eventually contract "the coronavirus." That's 160 million people.
That's the bad news. The good news is that of those 160 million, 90% or ~145 million will have little to no symptoms at all.
The bad news is that 15 million people will have serious symptoms and require intensive medical care. Of those 15 million, 5 million will die.
The good news is that there are 4 million doctors and nurses in this country. And another 7-10 million people with sufficient training to act as effective proxies for the licensed caregivers I mentioned above. I.e. people who can evaluate cases, triage and administer medication and other palliative measures.
Good news: That's a nearly 1:1 match with those that need medical attention, in a worst-case scenario. Now of course not all will be available, so let's call it a 1:0.5 match.
Bad news is that there are nowhere near enough hospital beds in the US for the 15 million that need them (there are about 800,000 beds today in the US, down from 1.5 million in 1975, the result of the rise of "regional" medical centers and the closing of rural hospitals as a result)
Good news is, even if we did have the beds, hospitals are no places for the sick.
What we should do, I believe, is instigate at the federal level a massive program to facilitate self-quarantine and other effective prophylactic measures. Those include:
1. Federal job protections for anyone who self-quarantines. Meaning you cannot be fired or suffer punishment for job absences of up to a month when justified on a quarantine basis.
2. Very large no-interest loans and/or substantial tax advantages to any company which continues to pay its workers who self quarantine. This includes hourly minimum-wage workers on up.
3. Widespread closures of schools from kindergarten through graduate education. Again, with federal financial support to those institutions which voluntarily close
4. The mobilization of a traveling medical corps from the pool of individuals I mentioned above. This should come under military jurisdiction because of the logistical factors. Basically a wholesale mobilization of medical caregivers under military command. They would be transported on a case basis to those who are at-risk (the 10%) and require medical care. Think an armada of olive-drab schoolhouses (we can use some of the buses idled when the schools are closed) taking medical personnel door-to-door on a daily basis.
Numbers-wise each medical professional will visit two critical patients per day, every day. In their homes or other facilities where needed (i.e. skilled nursing facilities)
5. The rapid creation of a large-scale manufacturing base capable of turning out antibiotics and other palliative medication as well as necessary medical equipment (syringes, saline solution, drip bags, thermometers, etc.). The country is full of disused and/or abandoned factories that should be mobilized towards this effort.
6. Finally, a wide-scale public education program on how to limit transmission. Starts with no touching anyone. Washing your hands. Internal travel bans. Avoid congregation (church, sporting events, conferences, etc.)
March 1st, 2020:
Comparisons between today's coronavirus and the flu pandemic of 1918:
a. The human immune system appeared to over-react to the 1918 virus. This is why that flu so disproportionally attacked the young and healthy -- those with healthy immune systems were killed by their own immune system over-reacting. The death rate was skewed towards those with healthy immune systems.
b. This coronavirus appears to cause an under-reaction in the immune system. That is why there is such a skewing to asymptomatic and/or mild cases. However, in persons with already compromised immune systems (old people like me), it can make them sick enough that other pathogens take hold -- i.e. it opens the door for things that the immune system was (just barely) keeping at bay. That's why the death rate is skewed towards those with poor immune systems (old and/or underlying conditions)
The 1918 pandemic eventually infected a third of the US population. But it killed only about 2% of those who were infected. So in that regard (number killed vs. number infected) it was similar to today's coronavirus.
A big difference between the 1918 virus and today is that in 1918 there were no antibiotics. Ironically, due to the antibiotic supply chain being destroyed (because the antibiotic factories in China are all shut down) there may not be any antibiotics this time around, either.
Comparisons between today's coronavirus and the flu pandemic of 1918:
a. The human immune system appeared to over-react to the 1918 virus. This is why that flu so disproportionally attacked the young and healthy -- those with healthy immune systems were killed by their own immune system over-reacting. The death rate was skewed towards those with healthy immune systems.
b. This coronavirus appears to cause an under-reaction in the immune system. That is why there is such a skewing to asymptomatic and/or mild cases. However, in persons with already compromised immune systems (old people like me), it can make them sick enough that other pathogens take hold -- i.e. it opens the door for things that the immune system was (just barely) keeping at bay. That's why the death rate is skewed towards those with poor immune systems (old and/or underlying conditions)
The 1918 pandemic eventually infected a third of the US population. But it killed only about 2% of those who were infected. So in that regard (number killed vs. number infected) it was similar to today's coronavirus.
A big difference between the 1918 virus and today is that in 1918 there were no antibiotics. Ironically, due to the antibiotic supply chain being destroyed (because the antibiotic factories in China are all shut down) there may not be any antibiotics this time around, either.
March 3rd, 2020:
The good news is that due to the large number of people who are infected with no or mild symptoms, together with willful underreporting/under-testing in the US (and some other countries), the Coronavirus actual death rate may be well under 2%
Wash your hands, don’t touch your face, don’t touch anything someone else has touched
The good news is that due to the large number of people who are infected with no or mild symptoms, together with willful underreporting/under-testing in the US (and some other countries), the Coronavirus actual death rate may be well under 2%
Wash your hands, don’t touch your face, don’t touch anything someone else has touched
March 4th, 2020:
A pandemic is an extremely complex system. But, importantly, it is VERY sensitive to small perturbations in its opportunities to spread.
In particular, all it takes to halt COVID-19 is a 30% reduction in person-to-person contact and the whole system is saved.
So, today, think about that third of your meetings with other people that you can blow off. And do it.
A pandemic is an extremely complex system. But, importantly, it is VERY sensitive to small perturbations in its opportunities to spread.
In particular, all it takes to halt COVID-19 is a 30% reduction in person-to-person contact and the whole system is saved.
So, today, think about that third of your meetings with other people that you can blow off. And do it.
March 6th, 2020:
New COVID-19 (coronavirus) data:
New study from China indicates that children contract the virus at the same rate as adults -- children are not "immune" as some have said. However, children are most likely to have mild symptoms. This has implications for prophylactic school closings (see more, below).
There is no evidence to support large numbers of asymptomatic patients. Virtually all asymptomatic individuals who are infected will develop symptoms within two days.
Median time to recovery is 32 days. Shorter in young people (25 days) and longer in old people (36 days)
School closings: In countries and localities that have already initiated school closings the social effect is profound. Parents are scrambling to find people to look after their children while they remain at work. Moreover there is significant disruption to the educational process. Not clear how or if that can be caught up
Governments are stepping in: Japan is subsidizing companies to offset the cost of having workers stay home caring for children. France is paying the wages of people (up to 14 days) who have to stay home either to self-isolate or to tend for sick children.
There are also already proposals in France to have the government inject $30 billion Euros (equivalent of $160 billion dollars when adjusted for population) into its economy as part of a program to repatriate the manufacture of goods that France is currently importing.
The United States has none of the social safety net architecture, including a single payer healthcare system, of the other developed countries and is particularly ill equipped for this crisis. Expect the lived experience here to be significantly worse than the lived experience in the other developed nations.
Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts
New COVID-19 (coronavirus) data:
New study from China indicates that children contract the virus at the same rate as adults -- children are not "immune" as some have said. However, children are most likely to have mild symptoms. This has implications for prophylactic school closings (see more, below).
There is no evidence to support large numbers of asymptomatic patients. Virtually all asymptomatic individuals who are infected will develop symptoms within two days.
Median time to recovery is 32 days. Shorter in young people (25 days) and longer in old people (36 days)
School closings: In countries and localities that have already initiated school closings the social effect is profound. Parents are scrambling to find people to look after their children while they remain at work. Moreover there is significant disruption to the educational process. Not clear how or if that can be caught up
Governments are stepping in: Japan is subsidizing companies to offset the cost of having workers stay home caring for children. France is paying the wages of people (up to 14 days) who have to stay home either to self-isolate or to tend for sick children.
There are also already proposals in France to have the government inject $30 billion Euros (equivalent of $160 billion dollars when adjusted for population) into its economy as part of a program to repatriate the manufacture of goods that France is currently importing.
The United States has none of the social safety net architecture, including a single payer healthcare system, of the other developed countries and is particularly ill equipped for this crisis. Expect the lived experience here to be significantly worse than the lived experience in the other developed nations.
Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts
March 6th, 2020:
Plague Hall of Fame:
Plague of Athens. 430-426BC. "Typhoid fever." Caused by bacteria (salmonella)
Kills a quarter of the population of Athens. Would have killed more if it was less virulent but ended up killing people at a faster rate than they could spread it.
--
Antonine Plague. 165-180AD. Smallpox. Kills a quarter of those infected. At height, as many as 5,000 a day dying in Rome.
--
First Plague Pandemic: 541-542 AD. "Plague of Justinian" (the Roman Emperor at the time, who also contracted it). Caused by bacteria, Yersinia pestis, carried by rats who were carried in ships. Flea bites rat, then flea bites human. Also extremely contagious human/human.
Kills half of all the people in the Roman Empire. 10,000 deaths a day in Constantinople (now Istanbul)
--
Second Plague Pandemic: 1334-1352 AD. "Black Death". Also caused by Yersinia pestis (i.e. bacteriological). Originates in China but is eventually spread to Europe through trade (rat-infested ships) and then worldwide.
Kills half the people in Europe.
--
Third Plague Pandemic: 1866-1960s. Also caused by, you guessed it, Yersinia pestis. Also originated in China & carried around the world in ships (rats & flea-infested cargo)
Kills 10 million people in India alone.
--
Influenza pandemic. 1918-1920. "Spanish Flu." Virus, however death caused by bacteriological secondary infection (pneumonia).
Infects 500 million people (~ one third of the world's population (1.8 billion at the time)). Kills as many as 100 million.
***
The discovery of antibiotics effectively put an end to Yersinia pestis, ending the "Black Death" type plagues and greatly reducing the consequences of secondary bacteriological infections in virus-caused diseases (i.e. the influenza pandemic of 1918).
Trivia: The first widely-known vaccination was a smallpox vaccination. Created by collecting scab material from those with smallpox, drying the scabs, and then grinding them into powder. Scab powder, containing dead smallpox virus, then inhaled into the nose.
Later refined into a real vaccine by Edward Jenner in 1796. Jenner collected pus from cows infected by cowpox and injected it into humans. Cowpox is similar enough genetically to smallpox that the immune system's learned reaction to cowpox is also effective against smallpox
Plague Hall of Fame:
Plague of Athens. 430-426BC. "Typhoid fever." Caused by bacteria (salmonella)
Kills a quarter of the population of Athens. Would have killed more if it was less virulent but ended up killing people at a faster rate than they could spread it.
--
Antonine Plague. 165-180AD. Smallpox. Kills a quarter of those infected. At height, as many as 5,000 a day dying in Rome.
--
First Plague Pandemic: 541-542 AD. "Plague of Justinian" (the Roman Emperor at the time, who also contracted it). Caused by bacteria, Yersinia pestis, carried by rats who were carried in ships. Flea bites rat, then flea bites human. Also extremely contagious human/human.
Kills half of all the people in the Roman Empire. 10,000 deaths a day in Constantinople (now Istanbul)
--
Second Plague Pandemic: 1334-1352 AD. "Black Death". Also caused by Yersinia pestis (i.e. bacteriological). Originates in China but is eventually spread to Europe through trade (rat-infested ships) and then worldwide.
Kills half the people in Europe.
--
Third Plague Pandemic: 1866-1960s. Also caused by, you guessed it, Yersinia pestis. Also originated in China & carried around the world in ships (rats & flea-infested cargo)
Kills 10 million people in India alone.
--
Influenza pandemic. 1918-1920. "Spanish Flu." Virus, however death caused by bacteriological secondary infection (pneumonia).
Infects 500 million people (~ one third of the world's population (1.8 billion at the time)). Kills as many as 100 million.
***
The discovery of antibiotics effectively put an end to Yersinia pestis, ending the "Black Death" type plagues and greatly reducing the consequences of secondary bacteriological infections in virus-caused diseases (i.e. the influenza pandemic of 1918).
Trivia: The first widely-known vaccination was a smallpox vaccination. Created by collecting scab material from those with smallpox, drying the scabs, and then grinding them into powder. Scab powder, containing dead smallpox virus, then inhaled into the nose.
Later refined into a real vaccine by Edward Jenner in 1796. Jenner collected pus from cows infected by cowpox and injected it into humans. Cowpox is similar enough genetically to smallpox that the immune system's learned reaction to cowpox is also effective against smallpox
March 6th, 2020:
Some more information from the paper I mentioned earlier:
Shenzen study covered: 391 confirmed SARS-CoV-2 cases and 1286 people who had had "close contact" with one of those cases.
Symptom based cases identified by presentation of clinical symptoms. Contact based cases identified as being in contact with an infected person than then confirmed to be infected themselves through laboratory test.
Ninety-one percent of those infected in the survey had either mild or moderate symptoms (see definitions below). Only 9% were severe.
In cases identified by symptoms, 88% had fever. In cases identified by contact, 70% had fever.
Cases are broken down by severity: mild, moderate or severe.
Fever, respiratory symptoms and radiological evidence of pneumonia are three factors that earn a designation of "moderate" symptoms
Severe symptoms include septic shock, need for mechanical ventilator, blood oxygen < 94%, and multiple organ dysfunction.
Anything else is characterized as mild.
Household "secondary attack" (transmission) is 15%. I.e. 15% of the people living in a household with an infected person contracted the virus.
"We further show that children are at similar risk of infection as the general population"
Generally the older you are the more severe your symptoms will be. However, it is not until you get to be 60 or older that it really diverges.
Median incubation (time between when you get infected and start to show symptoms: 5 days. At 14 days after infection, 95% of people will show symptoms.
Median time to recovery is 32 days.
In other words, you get the disease quickly but it takes a long time to be rid of it.
Outside of household transmission (15%), 10% of those with a close contact with an infected individual will become infected themselves.
No significant association between age and probability of infection.
OBSERVED R0 NUMBER WAS 0.4. This is the number on a heavily surveilled population.
"In Shenzhen, SARS-CoV-2 transmission is most likely between very close contacts, such as individuals sharing a household. However, even in this group less than 1 in 6 contacts were infected; and, overall, we observed far less than one (0.4) onward transmission per primary case. "
"It is, likewise, impossible to identify every potential contact an individual has, so contact tracing focuses on those close contacts most likely to be infected; hence our observed R is assuredly less than the true R in the population. "
Some more information from the paper I mentioned earlier:
Shenzen study covered: 391 confirmed SARS-CoV-2 cases and 1286 people who had had "close contact" with one of those cases.
Symptom based cases identified by presentation of clinical symptoms. Contact based cases identified as being in contact with an infected person than then confirmed to be infected themselves through laboratory test.
Ninety-one percent of those infected in the survey had either mild or moderate symptoms (see definitions below). Only 9% were severe.
In cases identified by symptoms, 88% had fever. In cases identified by contact, 70% had fever.
Cases are broken down by severity: mild, moderate or severe.
Fever, respiratory symptoms and radiological evidence of pneumonia are three factors that earn a designation of "moderate" symptoms
Severe symptoms include septic shock, need for mechanical ventilator, blood oxygen < 94%, and multiple organ dysfunction.
Anything else is characterized as mild.
Household "secondary attack" (transmission) is 15%. I.e. 15% of the people living in a household with an infected person contracted the virus.
"We further show that children are at similar risk of infection as the general population"
Generally the older you are the more severe your symptoms will be. However, it is not until you get to be 60 or older that it really diverges.
Median incubation (time between when you get infected and start to show symptoms: 5 days. At 14 days after infection, 95% of people will show symptoms.
Median time to recovery is 32 days.
In other words, you get the disease quickly but it takes a long time to be rid of it.
Outside of household transmission (15%), 10% of those with a close contact with an infected individual will become infected themselves.
No significant association between age and probability of infection.
OBSERVED R0 NUMBER WAS 0.4. This is the number on a heavily surveilled population.
"In Shenzhen, SARS-CoV-2 transmission is most likely between very close contacts, such as individuals sharing a household. However, even in this group less than 1 in 6 contacts were infected; and, overall, we observed far less than one (0.4) onward transmission per primary case. "
"It is, likewise, impossible to identify every potential contact an individual has, so contact tracing focuses on those close contacts most likely to be infected; hence our observed R is assuredly less than the true R in the population. "
March 7th, 2020:
This thing is about to explode. With spring break coming up week after next most responsible thing to do is to close Iu and mccsc and rbb [local school systems] next week. That gives two weeks for all of the infected to develop symptoms.
It would keep it under control and within the capacity of the local heath resources. Otherwise it will be overwhelming
This thing is about to explode. With spring break coming up week after next most responsible thing to do is to close Iu and mccsc and rbb [local school systems] next week. That gives two weeks for all of the infected to develop symptoms.
It would keep it under control and within the capacity of the local heath resources. Otherwise it will be overwhelming
March 7th, 2020:
Took the most recent COVID-19 (coronavirus) data and imported it into a spreadsheet. Here are the results.
The methodology is straight-forward: Number dead as a percentage of the number recovered+number dead. That means that the places listed below with 100% have had no one who contracted the disease recover and had one or more people who contracted the disease die.
Note that the mean time to recovery is 32 days. So those places where no one has recovered may not have had the infection long enough for anyone to recover but have had it long enough for someone to die.
Average worldwide death rate is currently 13%
Place: Death Rate
------------------
Netherlands: 100%
Iraq: 100%
San Marino: 100%
Snohomish County, US: 100%
Placer County, CA: 100%
Western Australia: 100%
King County, WA: 92%
Spain: 71%
United States: 68%
Phillippines: 50%
France: 43%
Italy: 27%
Switzerland: 25%
South Korea: 24%
UK: 20%
New South Wales (Australia): 20%
Diamond Princess Cruise: 13%
Iran: 12%
Japan: 12%
Taiwan: 8%
Mainland China (total): 5%
Hong Kong: 4%
Thailand: 3%
Germany: 0%
Singapore: 0%
India: 0%
Took the most recent COVID-19 (coronavirus) data and imported it into a spreadsheet. Here are the results.
The methodology is straight-forward: Number dead as a percentage of the number recovered+number dead. That means that the places listed below with 100% have had no one who contracted the disease recover and had one or more people who contracted the disease die.
Note that the mean time to recovery is 32 days. So those places where no one has recovered may not have had the infection long enough for anyone to recover but have had it long enough for someone to die.
Average worldwide death rate is currently 13%
Place: Death Rate
------------------
Netherlands: 100%
Iraq: 100%
San Marino: 100%
Snohomish County, US: 100%
Placer County, CA: 100%
Western Australia: 100%
King County, WA: 92%
Spain: 71%
United States: 68%
Phillippines: 50%
France: 43%
Italy: 27%
Switzerland: 25%
South Korea: 24%
UK: 20%
New South Wales (Australia): 20%
Diamond Princess Cruise: 13%
Iran: 12%
Japan: 12%
Taiwan: 8%
Mainland China (total): 5%
Hong Kong: 4%
Thailand: 3%
Germany: 0%
Singapore: 0%
India: 0%
March 7th, 2020:
The data that is beginning to emerge about the COVID-19 disease is: it is extremely deadly, irrespective of age or underlying conditions.
It is also fairly contagious, although not especially so.
What that means is that we need to put everything we can towards preventing infection. Practically, that means that each of us on an individual level has a responsibility to everyone else, including our families, to practice extreme isolation and extreme cleanliness.
It is NOT ok to not wash your hands. It is NOT ok to leave your home if you have any suspicion that you may have come in contact with the virus. It is NOT ok to attend any social gathering that is not absolutely necessary.
It's probably not OK to go to school at this point. And in a couple days, not OK to go to work, either.
The data that is beginning to emerge about the COVID-19 disease is: it is extremely deadly, irrespective of age or underlying conditions.
It is also fairly contagious, although not especially so.
What that means is that we need to put everything we can towards preventing infection. Practically, that means that each of us on an individual level has a responsibility to everyone else, including our families, to practice extreme isolation and extreme cleanliness.
It is NOT ok to not wash your hands. It is NOT ok to leave your home if you have any suspicion that you may have come in contact with the virus. It is NOT ok to attend any social gathering that is not absolutely necessary.
It's probably not OK to go to school at this point. And in a couple days, not OK to go to work, either.
March 11th, 2020:
Excellent analysis. What this shows is:
1. The importance of self-quarantine and vigorous social distancing commencing immediately. It is beyond my comprehension to understand why the schools, including IU, have not shut down. Every day is huge. Every day earlier that things get shut down has a dramatic effect on the contagion.
2. How quickly the system responds to a lockdown. China's new cases began an immediate decline within 24 hours of the lockdown there.
https://medium.com/…/coronavirus-act-today-or-people-will-d…
3. It is everywhere here. Official numbers of the infected are off by an order of magnitude. For instance, Washington State has 16,000 infected
Excellent analysis. What this shows is:
1. The importance of self-quarantine and vigorous social distancing commencing immediately. It is beyond my comprehension to understand why the schools, including IU, have not shut down. Every day is huge. Every day earlier that things get shut down has a dramatic effect on the contagion.
2. How quickly the system responds to a lockdown. China's new cases began an immediate decline within 24 hours of the lockdown there.
https://medium.com/…/coronavirus-act-today-or-people-will-d…
3. It is everywhere here. Official numbers of the infected are off by an order of magnitude. For instance, Washington State has 16,000 infected
March 11, 2020:
Denmark just closed all schools and universities. Also ordered all public sector employees to remain at home starting Friday.
Denmark just closed all schools and universities. Also ordered all public sector employees to remain at home starting Friday.
March 12th, 2020:
Good morning.
Social Distancing
———————————
1. Under no circumstances should you touch anyone else nor touch anything they have touched without precaution, such as immediately sanitizing your hands.
2. As much as humanly possible, do not approach closer than 6’ (six feet) to another person. The virus is spread by liquid droplets and a sneeze or a cough from someone else will radiate no more than six feet from them, after which the virus will fall to the ground.
3. The virus can live on metal surfaces, such as counter tops, door knobs/handles/etc. for at least three days. Regularly wipe your door handles @ home if people from outside are touching them. If you must touch a door handle with your bare hands, try and immediately wash them or apply hand sanitizer
Medications
----------------
4. There is evidence that ACE inhibitors, such as found in many blood pressure medicines, prevent or slow pneumonia progression. So if you are taking such blood pressure medications, keep doing it.
[NOTE THIS INFORMATION IS IN QUESTION, NOW I BELIEVE THE OPPOSITE]
5. Likewise there is good evidence that large amounts of vitamin C are beneficial. This is controversial but since it’s not possible to overdose on vitamin C, if you have it, take it. The Chinese are doing clinical studies with injections of 30,000mg of vitamin C and seeing some hopeful results.
6. Allergy medicines such as Zyrtec and Allegra are very helpful in keeping lungs “dry.” Even if you are not seeing/feeling allergy symptoms, a daily prophylactic dose of a 24 hour allergy medication is very good idea as a guard against pneumonia
7. Have ibuprofen, aspirin, Tylenol handy. If you develop a headache/fever/etc. rotate among them as necessary.
Health Care System
—————————————
8. The US health care system will very soon collapse as it is overwhelmed with serious cases. What that means is that it is critically important to do everything you can to not need any kind of structured care. I.e. practice aggressive social distancing and keep yourself healthy through prophylactic medications and exercise,. Be careful with exercise however that you do not suffer some secondary injury like a fall that would require medical attention. Hospitals and clinics will be soaked with the virus and a trip to one is a very good way to contract the virus.
9. We should expect that 50% of the US population will eventually contract the virus with a 5% fatality rate (the latter due to a lack of immediate lockdown/social distancing coupled with the poor state of our health care system). That’s roughly 6 million dead and 26 million more who will become critically ill (but eventually recover). Most of that will be heavily skewed towards those 65 and older.
10. Children do not (currently) seem to suffer from the virus. However, they are a significant vector (they are carriers). Avoid children like the plague. The virus will probably mutate and it is likely that a mutation may affect children more directly in the future. All gatherings of children should be stringently avoided. Schools must be closed immediately.
11. Although we can probably not prevent the virus from infecting most of us eventually, we can alter the timeframe over which it does significantly with social distancing/quarantine, With no distancing/quarantine the infection rate will double every 24 hours — i.e. every day twice as many people will contract. With aggressive distancing/quarantine that rate is fairly easily brought under 1 (“R-nought”) which causes the infection rate to rapidly drop to zero. This is what was seen in China where the cases of new infections dropped immediately (within 24 hours) of the “lockdown” and has since fallen to effectively zero.
Shopping
——————
12. Avoid fresh produce, vegetables, fruits, etc. and any other food product that is subject to high amounts of human touching.
13. Stock up on non-perishable items (canned items like soup, boxed dry goods that are mechanically packed (crackers, etc.)). It is unlikely that such packaging itself would be contaminated but use best practices nonetheless — i.e. wash hands after handling boxes, cans, etc. At least for a few days after you get them. Within three-five days after they come home, any residual virus should be dead.
14. Stock up on vitamins (see medications, above) as a supplement for what you are not getting via fruits and vegetables.
Good morning.
Social Distancing
———————————
1. Under no circumstances should you touch anyone else nor touch anything they have touched without precaution, such as immediately sanitizing your hands.
2. As much as humanly possible, do not approach closer than 6’ (six feet) to another person. The virus is spread by liquid droplets and a sneeze or a cough from someone else will radiate no more than six feet from them, after which the virus will fall to the ground.
3. The virus can live on metal surfaces, such as counter tops, door knobs/handles/etc. for at least three days. Regularly wipe your door handles @ home if people from outside are touching them. If you must touch a door handle with your bare hands, try and immediately wash them or apply hand sanitizer
Medications
----------------
4. There is evidence that ACE inhibitors, such as found in many blood pressure medicines, prevent or slow pneumonia progression. So if you are taking such blood pressure medications, keep doing it.
[NOTE THIS INFORMATION IS IN QUESTION, NOW I BELIEVE THE OPPOSITE]
5. Likewise there is good evidence that large amounts of vitamin C are beneficial. This is controversial but since it’s not possible to overdose on vitamin C, if you have it, take it. The Chinese are doing clinical studies with injections of 30,000mg of vitamin C and seeing some hopeful results.
6. Allergy medicines such as Zyrtec and Allegra are very helpful in keeping lungs “dry.” Even if you are not seeing/feeling allergy symptoms, a daily prophylactic dose of a 24 hour allergy medication is very good idea as a guard against pneumonia
7. Have ibuprofen, aspirin, Tylenol handy. If you develop a headache/fever/etc. rotate among them as necessary.
Health Care System
—————————————
8. The US health care system will very soon collapse as it is overwhelmed with serious cases. What that means is that it is critically important to do everything you can to not need any kind of structured care. I.e. practice aggressive social distancing and keep yourself healthy through prophylactic medications and exercise,. Be careful with exercise however that you do not suffer some secondary injury like a fall that would require medical attention. Hospitals and clinics will be soaked with the virus and a trip to one is a very good way to contract the virus.
9. We should expect that 50% of the US population will eventually contract the virus with a 5% fatality rate (the latter due to a lack of immediate lockdown/social distancing coupled with the poor state of our health care system). That’s roughly 6 million dead and 26 million more who will become critically ill (but eventually recover). Most of that will be heavily skewed towards those 65 and older.
10. Children do not (currently) seem to suffer from the virus. However, they are a significant vector (they are carriers). Avoid children like the plague. The virus will probably mutate and it is likely that a mutation may affect children more directly in the future. All gatherings of children should be stringently avoided. Schools must be closed immediately.
11. Although we can probably not prevent the virus from infecting most of us eventually, we can alter the timeframe over which it does significantly with social distancing/quarantine, With no distancing/quarantine the infection rate will double every 24 hours — i.e. every day twice as many people will contract. With aggressive distancing/quarantine that rate is fairly easily brought under 1 (“R-nought”) which causes the infection rate to rapidly drop to zero. This is what was seen in China where the cases of new infections dropped immediately (within 24 hours) of the “lockdown” and has since fallen to effectively zero.
Shopping
——————
12. Avoid fresh produce, vegetables, fruits, etc. and any other food product that is subject to high amounts of human touching.
13. Stock up on non-perishable items (canned items like soup, boxed dry goods that are mechanically packed (crackers, etc.)). It is unlikely that such packaging itself would be contaminated but use best practices nonetheless — i.e. wash hands after handling boxes, cans, etc. At least for a few days after you get them. Within three-five days after they come home, any residual virus should be dead.
14. Stock up on vitamins (see medications, above) as a supplement for what you are not getting via fruits and vegetables.
March 12th, 2020:
I was asked to provide some recommendations for a facility that serves an at-risk population. This was my response:
"If at all possible, I would try and obtain at least one non-contact IR thermometer (the kind you can aim at someone's forehead without touching them) and disallow anyone in the facilities with an elevated temperature. Of course you are going to have to find an alternate way of getting their food to them.
Also if at all possible, obtain a sanitation station (or a hundred) at all entrances to the facilities. Either a gel dispenser or a sanitizing wipe dispenser. Require that everyone entering wipe their hands with it on both entry and exit
Any and all surfaces should receive some kind of sanitary spray (alcohol or chlorine+water) multiple times a day
Oh, and in addition to temperature tests no one exhibiting any symptoms of coughing or sneezing or runny nose in the facility. Infected individuals will spread it to the facility either by touching something (which is why the hand wipe on entry is so important) or by coughing or sneezing on something
If you have anywhere where people queue up (a line) in the facility, post signs telling people to remain at least 4 feet away from one another and preferably 6. At 6' separation someone with COVID-19 cannot spread it to another person if they sneeze or cough.”
I was asked to provide some recommendations for a facility that serves an at-risk population. This was my response:
"If at all possible, I would try and obtain at least one non-contact IR thermometer (the kind you can aim at someone's forehead without touching them) and disallow anyone in the facilities with an elevated temperature. Of course you are going to have to find an alternate way of getting their food to them.
Also if at all possible, obtain a sanitation station (or a hundred) at all entrances to the facilities. Either a gel dispenser or a sanitizing wipe dispenser. Require that everyone entering wipe their hands with it on both entry and exit
Any and all surfaces should receive some kind of sanitary spray (alcohol or chlorine+water) multiple times a day
Oh, and in addition to temperature tests no one exhibiting any symptoms of coughing or sneezing or runny nose in the facility. Infected individuals will spread it to the facility either by touching something (which is why the hand wipe on entry is so important) or by coughing or sneezing on something
If you have anywhere where people queue up (a line) in the facility, post signs telling people to remain at least 4 feet away from one another and preferably 6. At 6' separation someone with COVID-19 cannot spread it to another person if they sneeze or cough.”
March 12th, 2020:
Iranian burial trenches for COVID-19 fatalities. Are we self-quarantining, yet?
Iranian burial trenches for COVID-19 fatalities. Are we self-quarantining, yet?

March 12th, 2020:
From reports that I am receiving, today is the day that COVID-19 symptoms exploded in Bloomington.
From reports that I am receiving, today is the day that COVID-19 symptoms exploded in Bloomington.
March 12th, 2020:
From my friend, Sarah Comey Cluff:
"UCSF COVID 19 updates (much thanks to PV): #coronavirus info:
“University of California, San Francisco BioHub Panel on COVID-19
March 10, 2020
• Panelists
• Joe DeRisi: UCSF’s top infectious disease researcher. Co-president of ChanZuckerberg BioHub (a JV involving UCSF / Berkeley / Stanford). Co-inventor of the chip used in SARS epidemic.
• Emily Crawford: COVID task force director. Focused on diagnostics
• Cristina Tato: Rapid Response Director. Immunologist.
• Patrick Ayescue: Leading outbreak response and surveillance. Epidemiologist.
• Chaz Langelier: UCSF Infectious Disease doc
What’s below are essentially direct quotes from the panelists. I bracketed the few things that are not quotes.
• Top takeaways
• At this point, we are past containment. Containment is basically futile. Our containment efforts won’t reduce the number who get infected in the US.
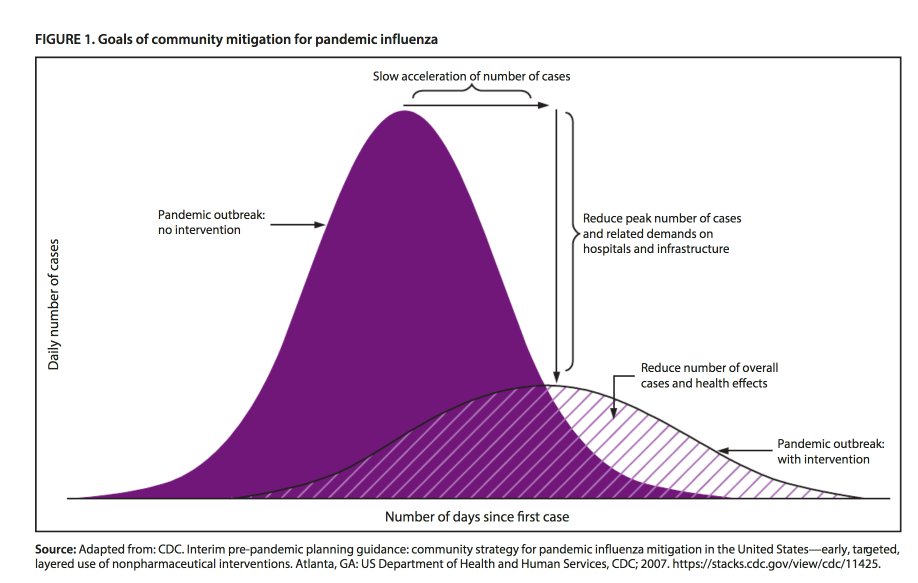
• Now we’re just trying to slow the spread, to help healthcare providers deal with the demand peak. In other words, the goal of containment is to "flatten the curve", to lower the peak of the surge of demand that will hit healthcare providers. And to buy time, in hopes a drug can be developed.
• How many in the community already have the virus? No one knows.
• We are moving from containment to care.
• We in the US are currently where Italy was a week ago. We see nothing to say we will be substantially different.
• 40-70% of the US population will be infected over the next 12-18 months. After that level you can start to get herd immunity. Unlike flu this is entirely novel to humans, so there is no latent immunity in the global population.
• [We used their numbers to work out a guesstimate of deaths— indicating about 1.5 million Americans may die. The panelists did not disagree with our estimate. This compares to seasonal flu’s average of 50K Americans per year. Assume 50% of US population, that’s 160M people infected. With 1% mortality rate that's 1.6M Americans die over the next 12-18 months.]
• The fatality rate is in the range of 10X flu.
• This assumes no drug is found effective and made available.
• The death rate varies hugely by age. Over age 80 the mortality rate could be 10-15%. [See chart by age Signe found online, attached at bottom.]
• Don’t know whether COVID-19 is seasonal but if is and subsides over the summer, it is likely to roar back in fall as the 1918 flu did
• I can only tell you two things definitively. Definitively it’s going to get worse before it gets better. And we'll be dealing with this for the next year at least. Our lives are going to look different for the next year.
• What should we do now? What are you doing for your family?
• Appears one can be infectious before being symptomatic. We don’t know how infectious before symptomatic, but know that highest level of virus prevalence coincides with symptoms. We currently think folks are infectious 2 days before through 14 days after onset of symptoms (T-2 to T+14 onset).
• How long does the virus last?
• On surfaces, best guess is 4-20 hours depending on surface type (maybe a few days) but still no consensus on this
• The virus is very susceptible to common anti-bacterial cleaning agents: bleach, hydrogen peroxide, alcohol-based.
• Avoid concerts, movies, crowded places.
• We have cancelled business travel.
• Do the basic hygiene, eg hand washing and avoiding touching face.
• Stockpile your critical prescription medications. Many pharma supply chains run through China. Pharma companies usually hold 2-3 months of raw materials, so may run out given the disruption in China’s manufacturing.
• Pneumonia shot might be helpful. Not preventative of COVID-19, but reduces your chance of being weakened, which makes COVID-19 more dangerous.
• Get a flu shot next fall. Not preventative of COVID-19, but reduces your chance of being weakened, which makes COVID-19 more dangerous.
• We would say “Anyone over 60 stay at home unless it’s critical”. CDC toyed with idea of saying anyone over 60 not travel on commercial airlines.
• We at UCSF are moving our “at-risk” parents back from nursing homes, etc. to their own homes. Then are not letting them out of the house. The other members of the family are washing hands the moment they come in.
• Three routes of infection
• Hand to mouth / face
• Aerosol transmission
• Fecal oral route
• What if someone is sick?
• If someone gets sick, have them stay home and socially isolate. There is very little you can do at a hospital that you couldn’t do at home. Most cases are mild. But if they are old or have lung or cardio-vascular problems, read on.
• If someone gets quite sick who is old (70+) or with lung or cardio-vascular problems, take them to the ER.
• There is no accepted treatment for COVID-19. The hospital will give supportive care (eg IV fluids, oxygen) to help you stay alive while your body fights the disease. ie to prevent sepsis.
• If someone gets sick who is high risk (eg is both old and has lung/cardio-vascular problems), you can try to get them enrolled for “compassionate use" of Remdesivir, a drug that is in clinical trial at San Francisco General and UCSF, and in China. Need to find a doc there in order to ask to enroll. Remdesivir is an anti-viral from Gilead that showed effectiveness against MERS in primates and is being tried against COVID-19. If the trials succeed it might be available for next winter as production scales up far faster for drugs than for vaccines. [More I found online.]
• Why is the fatality rate much higher for older adults?
• Your immune system declines past age 50
• Fatality rate tracks closely with “co-morbidity”, ie the presence of other conditions that compromise the patient’s hearth, especially respiratory or cardio-vascular illness. These conditions are higher in older adults.
• Risk of pneumonia is higher in older adults.
• What about testing to know if someone has COVID-19?
• Bottom line, there is not enough testing capacity to be broadly useful. Here’s why.
• Currently, there is no way to determine what a person has other than a PCR test. No other test can yet distinguish "COVID-19 from flu or from the other dozen respiratory bugs that are circulating”.
• A Polymerase Chain Reaction (PCR) test can detect COVID-19’s RNA. However they still don’t have confidence in the test’s specificity, ie they don’t know the rate of false negatives.
• The PCR test requires kits with reagents and requires clinical labs to process the kits.
• While the kits are becoming available, the lab capacity is not growing.
• The leading clinical lab firms, Quest and Labcore have capacity to process 1000 kits per day. For the nation.
• Expanding processing capacity takes “time, space, and equipment.” And certification. ie it won’t happen soon.
• UCSF and UCBerkeley have donated their research labs to process kits. But each has capacity to process only 20-40 kits per day. And are not clinically certified.
• Novel test methods are on the horizon, but not here now and won’t be at any scale to be useful for the present danger.
• How well is society preparing for the impact?
• Local hospitals are adding capacity as we speak. UCSF’s Parnassus campus has erected “triage tents” in a parking lot. They have converted a ward to “negative pressure” which is needed to contain the virus. They are considering re-opening the shuttered Mt Zion facility.
• If COVID-19 affected children then we would be seeing mass departures of families from cities. But thankfully now we know that kids are not affected.
• School closures are one the biggest societal impacts. We need to be thoughtful before we close schools, especially elementary schools because of the knock-on effects. If elementary kids are not in school then some hospital staff can’t come to work, which decreases hospital capacity at a time of surging demand for hospital services.
• Public Health systems are prepared to deal with short-term outbreaks that last for weeks, like an outbreak of meningitis. They do not have the capacity to sustain for outbreaks that last for months. Other solutions will have to be found.
• What will we do to handle behavior changes that can last for months?
• Many employees will need to make accommodations for elderly parents and those with underlying conditions and immune-suppressed.
• Kids home due to school closures
• [Dr. DeRisi had to leave the meeting for a call with the governor’s office. When he returned we asked what the call covered.] The epidemiological models the state is using to track and trigger action. The state is planning at what point they will take certain actions. ie what will trigger an order to cease any gatherings of over 1000 people.
• Where do you find reliable news?
• The John Hopkins Center for Health Security site. Which posts daily updates. The site says you can sign up to receive a daily newsletter on COVID-19 by email. [I tried and the page times out due to high demand. After three more tries I was successful in registering for the newsletter.]
• The New York Times is good on scientific accuracy.
• Observations on China
• Unlike during SARS, China’s scientists are publishing openly and accurately on COVID-19.
• While China’s early reports on incidence were clearly low, that seems to trace to their data management systems being overwhelmed, not to any bad intent.
• Wuhan has 4.3 beds per thousand while US has 2.8 beds per thousand. Wuhan built 2 additional hospitals in 2 weeks. Even so, most patients were sent to gymnasiums to sleep on cots.
• Early on no one had info on COVID-19. So China reacted in a way unique modern history, except in wartime.
• Every few years there seems another: SARS, Ebola, MERS, H1N1, COVID-19. Growing strains of antibiotic resistant bacteria. Are we in the twilight of a century of medicine’s great triumph over infectious disease?
• "We’ve been in a back and forth battle against viruses for a million years."
• But it would sure help if every country would shut down their wet markets.
• As with many things, the worst impact of COVID-19 will likely be in the countries with the least resources, eg Africa. See article on Wired magazine on sequencing of virus from Cambodia.”
From my friend, Sarah Comey Cluff:
"UCSF COVID 19 updates (much thanks to PV): #coronavirus info:
“University of California, San Francisco BioHub Panel on COVID-19
March 10, 2020
• Panelists
• Joe DeRisi: UCSF’s top infectious disease researcher. Co-president of ChanZuckerberg BioHub (a JV involving UCSF / Berkeley / Stanford). Co-inventor of the chip used in SARS epidemic.
• Emily Crawford: COVID task force director. Focused on diagnostics
• Cristina Tato: Rapid Response Director. Immunologist.
• Patrick Ayescue: Leading outbreak response and surveillance. Epidemiologist.
• Chaz Langelier: UCSF Infectious Disease doc
What’s below are essentially direct quotes from the panelists. I bracketed the few things that are not quotes.
• Top takeaways
• At this point, we are past containment. Containment is basically futile. Our containment efforts won’t reduce the number who get infected in the US.
• Now we’re just trying to slow the spread, to help healthcare providers deal with the demand peak. In other words, the goal of containment is to "flatten the curve", to lower the peak of the surge of demand that will hit healthcare providers. And to buy time, in hopes a drug can be developed.
• How many in the community already have the virus? No one knows.
• We are moving from containment to care.
• We in the US are currently where Italy was a week ago. We see nothing to say we will be substantially different.
• 40-70% of the US population will be infected over the next 12-18 months. After that level you can start to get herd immunity. Unlike flu this is entirely novel to humans, so there is no latent immunity in the global population.
• [We used their numbers to work out a guesstimate of deaths— indicating about 1.5 million Americans may die. The panelists did not disagree with our estimate. This compares to seasonal flu’s average of 50K Americans per year. Assume 50% of US population, that’s 160M people infected. With 1% mortality rate that's 1.6M Americans die over the next 12-18 months.]
• The fatality rate is in the range of 10X flu.
• This assumes no drug is found effective and made available.
• The death rate varies hugely by age. Over age 80 the mortality rate could be 10-15%. [See chart by age Signe found online, attached at bottom.]
• Don’t know whether COVID-19 is seasonal but if is and subsides over the summer, it is likely to roar back in fall as the 1918 flu did
• I can only tell you two things definitively. Definitively it’s going to get worse before it gets better. And we'll be dealing with this for the next year at least. Our lives are going to look different for the next year.
• What should we do now? What are you doing for your family?
• Appears one can be infectious before being symptomatic. We don’t know how infectious before symptomatic, but know that highest level of virus prevalence coincides with symptoms. We currently think folks are infectious 2 days before through 14 days after onset of symptoms (T-2 to T+14 onset).
• How long does the virus last?
• On surfaces, best guess is 4-20 hours depending on surface type (maybe a few days) but still no consensus on this
• The virus is very susceptible to common anti-bacterial cleaning agents: bleach, hydrogen peroxide, alcohol-based.
• Avoid concerts, movies, crowded places.
• We have cancelled business travel.
• Do the basic hygiene, eg hand washing and avoiding touching face.
• Stockpile your critical prescription medications. Many pharma supply chains run through China. Pharma companies usually hold 2-3 months of raw materials, so may run out given the disruption in China’s manufacturing.
• Pneumonia shot might be helpful. Not preventative of COVID-19, but reduces your chance of being weakened, which makes COVID-19 more dangerous.
• Get a flu shot next fall. Not preventative of COVID-19, but reduces your chance of being weakened, which makes COVID-19 more dangerous.
• We would say “Anyone over 60 stay at home unless it’s critical”. CDC toyed with idea of saying anyone over 60 not travel on commercial airlines.
• We at UCSF are moving our “at-risk” parents back from nursing homes, etc. to their own homes. Then are not letting them out of the house. The other members of the family are washing hands the moment they come in.
• Three routes of infection
• Hand to mouth / face
• Aerosol transmission
• Fecal oral route
• What if someone is sick?
• If someone gets sick, have them stay home and socially isolate. There is very little you can do at a hospital that you couldn’t do at home. Most cases are mild. But if they are old or have lung or cardio-vascular problems, read on.
• If someone gets quite sick who is old (70+) or with lung or cardio-vascular problems, take them to the ER.
• There is no accepted treatment for COVID-19. The hospital will give supportive care (eg IV fluids, oxygen) to help you stay alive while your body fights the disease. ie to prevent sepsis.
• If someone gets sick who is high risk (eg is both old and has lung/cardio-vascular problems), you can try to get them enrolled for “compassionate use" of Remdesivir, a drug that is in clinical trial at San Francisco General and UCSF, and in China. Need to find a doc there in order to ask to enroll. Remdesivir is an anti-viral from Gilead that showed effectiveness against MERS in primates and is being tried against COVID-19. If the trials succeed it might be available for next winter as production scales up far faster for drugs than for vaccines. [More I found online.]
• Why is the fatality rate much higher for older adults?
• Your immune system declines past age 50
• Fatality rate tracks closely with “co-morbidity”, ie the presence of other conditions that compromise the patient’s hearth, especially respiratory or cardio-vascular illness. These conditions are higher in older adults.
• Risk of pneumonia is higher in older adults.
• What about testing to know if someone has COVID-19?
• Bottom line, there is not enough testing capacity to be broadly useful. Here’s why.
• Currently, there is no way to determine what a person has other than a PCR test. No other test can yet distinguish "COVID-19 from flu or from the other dozen respiratory bugs that are circulating”.
• A Polymerase Chain Reaction (PCR) test can detect COVID-19’s RNA. However they still don’t have confidence in the test’s specificity, ie they don’t know the rate of false negatives.
• The PCR test requires kits with reagents and requires clinical labs to process the kits.
• While the kits are becoming available, the lab capacity is not growing.
• The leading clinical lab firms, Quest and Labcore have capacity to process 1000 kits per day. For the nation.
• Expanding processing capacity takes “time, space, and equipment.” And certification. ie it won’t happen soon.
• UCSF and UCBerkeley have donated their research labs to process kits. But each has capacity to process only 20-40 kits per day. And are not clinically certified.
• Novel test methods are on the horizon, but not here now and won’t be at any scale to be useful for the present danger.
• How well is society preparing for the impact?
• Local hospitals are adding capacity as we speak. UCSF’s Parnassus campus has erected “triage tents” in a parking lot. They have converted a ward to “negative pressure” which is needed to contain the virus. They are considering re-opening the shuttered Mt Zion facility.
• If COVID-19 affected children then we would be seeing mass departures of families from cities. But thankfully now we know that kids are not affected.
• School closures are one the biggest societal impacts. We need to be thoughtful before we close schools, especially elementary schools because of the knock-on effects. If elementary kids are not in school then some hospital staff can’t come to work, which decreases hospital capacity at a time of surging demand for hospital services.
• Public Health systems are prepared to deal with short-term outbreaks that last for weeks, like an outbreak of meningitis. They do not have the capacity to sustain for outbreaks that last for months. Other solutions will have to be found.
• What will we do to handle behavior changes that can last for months?
• Many employees will need to make accommodations for elderly parents and those with underlying conditions and immune-suppressed.
• Kids home due to school closures
• [Dr. DeRisi had to leave the meeting for a call with the governor’s office. When he returned we asked what the call covered.] The epidemiological models the state is using to track and trigger action. The state is planning at what point they will take certain actions. ie what will trigger an order to cease any gatherings of over 1000 people.
• Where do you find reliable news?
• The John Hopkins Center for Health Security site. Which posts daily updates. The site says you can sign up to receive a daily newsletter on COVID-19 by email. [I tried and the page times out due to high demand. After three more tries I was successful in registering for the newsletter.]
• The New York Times is good on scientific accuracy.
• Observations on China
• Unlike during SARS, China’s scientists are publishing openly and accurately on COVID-19.
• While China’s early reports on incidence were clearly low, that seems to trace to their data management systems being overwhelmed, not to any bad intent.
• Wuhan has 4.3 beds per thousand while US has 2.8 beds per thousand. Wuhan built 2 additional hospitals in 2 weeks. Even so, most patients were sent to gymnasiums to sleep on cots.
• Early on no one had info on COVID-19. So China reacted in a way unique modern history, except in wartime.
• Every few years there seems another: SARS, Ebola, MERS, H1N1, COVID-19. Growing strains of antibiotic resistant bacteria. Are we in the twilight of a century of medicine’s great triumph over infectious disease?
• "We’ve been in a back and forth battle against viruses for a million years."
• But it would sure help if every country would shut down their wet markets.
• As with many things, the worst impact of COVID-19 will likely be in the countries with the least resources, eg Africa. See article on Wired magazine on sequencing of virus from Cambodia.”
March 12th, 2020:
From a friend:
"Ohio officials believe more than 100,000 people in the state carry coronavirus, underscoring limited testing
Ohio officials said Thursday that more than 100,000 people in the state are believed to carry the novel coronavirus, reinforcing fears that infections are far more widespread in the United States than limited testing confirms.
“We know now, just the fact of community spread says that at least 1 percent, at the very least 1 percent of our population is carrying this virus in Ohio today,” said Amy Acton, director of the Ohio Department of Health."
From a friend:
"Ohio officials believe more than 100,000 people in the state carry coronavirus, underscoring limited testing
Ohio officials said Thursday that more than 100,000 people in the state are believed to carry the novel coronavirus, reinforcing fears that infections are far more widespread in the United States than limited testing confirms.
“We know now, just the fact of community spread says that at least 1 percent, at the very least 1 percent of our population is carrying this virus in Ohio today,” said Amy Acton, director of the Ohio Department of Health."
March 12th, 2020:
Expect everyone to contract COVID-19. Expect yourself to contract COVID-19.
Do everything you can to make it so that you don't contract it now. The more you can isolate, the more you can put getting it in the future. In the future there will be more resources, there may be a vaccine if you can put it off.
Hunker down. Wash your hands.
Expect everyone to contract COVID-19. Expect yourself to contract COVID-19.
Do everything you can to make it so that you don't contract it now. The more you can isolate, the more you can put getting it in the future. In the future there will be more resources, there may be a vaccine if you can put it off.
Hunker down. Wash your hands.
March 12th, 2020:
Evidence is that people are most infectious 2 days to three days after symptoms begin. In other words, if you contract COVID-19 you are most likely to pass it to others between two days before you show symptoms to three days after your symptoms began.
Around Bloomington I would say that makes the most infectious time beginning right now and will continue until a substantial number of become infected and that will take a month.
Wash your hands.
Evidence is that people are most infectious 2 days to three days after symptoms begin. In other words, if you contract COVID-19 you are most likely to pass it to others between two days before you show symptoms to three days after your symptoms began.
Around Bloomington I would say that makes the most infectious time beginning right now and will continue until a substantial number of become infected and that will take a month.
Wash your hands.
March 12th, 2020:
Aaaannndddd, MCCSC [local school system] shut down:
Monroe County Community School Corporation Closure
Aaaannndddd, MCCSC [local school system] shut down:
Monroe County Community School Corporation Closure
March 13th, 2020:
My mother just sent me these pictures of them putting up infection tents the University of California San Francisco medical campus, a few blocks from her home.
We should be doing the same here in Bloomington. Assembly Hall and the various school gymnasiums should be getting filled with cots, blankets, and triage areas right now.
My mother just sent me these pictures of them putting up infection tents the University of California San Francisco medical campus, a few blocks from her home.
We should be doing the same here in Bloomington. Assembly Hall and the various school gymnasiums should be getting filled with cots, blankets, and triage areas right now.

March 13th, 2020:
On the Herald-Times' [local newspaper] website right now. Absolutely unbelievably irresponsible.
On the Herald-Times' [local newspaper] website right now. Absolutely unbelievably irresponsible.
March 13th, 2020:
What I heard during the President's address today:
1. We placed a big order for ventilators. From who? How many?
2. Target, Walmart, CVS and Walgreens will make their parking lots available for drive-through testing. With what testing kits?
3. Pence devoting his time to telling the public how magnificent Trump's leadership has been, while not citing a single bit of evidence other than Trump told Pence and others to talk to the private sector.
4. Google is putting up a website with a FAQ and a self-diagnosis function that shunts you away from hospitals.
5. Drug testing companies no longer have to worry about red tape. Why wasn't that taken away two months ago, when any idiot could have seen this day coming? 6. None of this is Trump's fault.
What I heard during the President's address today:
1. We placed a big order for ventilators. From who? How many?
2. Target, Walmart, CVS and Walgreens will make their parking lots available for drive-through testing. With what testing kits?
3. Pence devoting his time to telling the public how magnificent Trump's leadership has been, while not citing a single bit of evidence other than Trump told Pence and others to talk to the private sector.
4. Google is putting up a website with a FAQ and a self-diagnosis function that shunts you away from hospitals.
5. Drug testing companies no longer have to worry about red tape. Why wasn't that taken away two months ago, when any idiot could have seen this day coming? 6. None of this is Trump's fault.
March 13th, 2020:
On the "Google" website that the president promised would soon be available:
1. The website is actually being created by a company called Verily, which is owned by Google. But it is not Google.
2. The website is specific to the Bay Area and functionality limited to the Bay Area is what they are planning on rolling out initially.
3. The president's characterization of the website as being "nationwide" is a lie.
4. The basic functionality of the website is a questionnaire of the form "Do you have a fever?" "Do you have a cough?" "Have you been to Italy?" etc. It's totally bare-bones.
5. It does not send you to any of the drive-through testing centers. Which is good, since they don't exist and are not likely to exist for a long time, if ever.
On the "Google" website that the president promised would soon be available:
1. The website is actually being created by a company called Verily, which is owned by Google. But it is not Google.
2. The website is specific to the Bay Area and functionality limited to the Bay Area is what they are planning on rolling out initially.
3. The president's characterization of the website as being "nationwide" is a lie.
4. The basic functionality of the website is a questionnaire of the form "Do you have a fever?" "Do you have a cough?" "Have you been to Italy?" etc. It's totally bare-bones.
5. It does not send you to any of the drive-through testing centers. Which is good, since they don't exist and are not likely to exist for a long time, if ever.
March 13th, 2020:
Oh, Johns Hopkins/WHO just posted todays numbers. I processed them.
Italy's death rate, this far into their crisis, is terrifying. They are running a nearly 50% death rate.
Oh, Johns Hopkins/WHO just posted todays numbers. I processed them.
Italy's death rate, this far into their crisis, is terrifying. They are running a nearly 50% death rate.
March 13th, 2020:
Ok, time for some good news. The reported infection rates, the ones on my graphs, lag the actual infection rates by about two weeks. In other words, the infection numbers that came out today for Italy (17,660) are what the actual infection #s were about two weeks ago.
Four days ago, Italy went on lockdown with people being fined if caught outside during the day. When China did the same thing two months ago, new infections rapidly declined within 24 hours.
That means that the rate of new infections in Italy most likely began to decline last Wednesday.
The experience in China tells us the under lockdown you can expect the # of new cases to drop to essentially zero within a month of the lockdown. That means that Italy's rate, so long as they maintain the lockdown, should be approximately zero by the second week in April. Italy should be able to emerge from the crisis perhaps by mid-May.
We are a couple of weeks behind Italy, meaning we're probably a couple of weeks before our own mandatory lockdown, after which the incidences of new infections should begin to drop precipitously and we could be at zero new infections by the beginning May, emerging perhaps by early July.
Ok, time for some good news. The reported infection rates, the ones on my graphs, lag the actual infection rates by about two weeks. In other words, the infection numbers that came out today for Italy (17,660) are what the actual infection #s were about two weeks ago.
Four days ago, Italy went on lockdown with people being fined if caught outside during the day. When China did the same thing two months ago, new infections rapidly declined within 24 hours.
That means that the rate of new infections in Italy most likely began to decline last Wednesday.
The experience in China tells us the under lockdown you can expect the # of new cases to drop to essentially zero within a month of the lockdown. That means that Italy's rate, so long as they maintain the lockdown, should be approximately zero by the second week in April. Italy should be able to emerge from the crisis perhaps by mid-May.
We are a couple of weeks behind Italy, meaning we're probably a couple of weeks before our own mandatory lockdown, after which the incidences of new infections should begin to drop precipitously and we could be at zero new infections by the beginning May, emerging perhaps by early July.
This is from Twitter. I found it particularly compelling in these days:
"Just want to repeat my core belief here that the spiritual lesson of the past four years is that individualism is bullshit, it hurt the very fabric of our souls, isolating ourselves emotionally hurts us more than it hurts anyone else, and all we ever have is each other.
And learn to be grateful for love when you get it, because despite what you think when you're young and arrogant and the world is throwing itself at your feet, it doesn't come around again as often as you may think and if you throw it away it doesn't come around again at all."
Quote is from Heidi Moore ( @moorehn on Twitter )
"Just want to repeat my core belief here that the spiritual lesson of the past four years is that individualism is bullshit, it hurt the very fabric of our souls, isolating ourselves emotionally hurts us more than it hurts anyone else, and all we ever have is each other.
And learn to be grateful for love when you get it, because despite what you think when you're young and arrogant and the world is throwing itself at your feet, it doesn't come around again as often as you may think and if you throw it away it doesn't come around again at all."
Quote is from Heidi Moore ( @moorehn on Twitter )
March 14th, 2020:
Very good news. The death rate in South Korea is coming down precipitously and the resolution rate is rising. This is good evidence that widespread testing can have a beneficial effect.
Four days ago the death rate in South Korea was 30%. Today it's just over 10%.
Very good news. The death rate in South Korea is coming down precipitously and the resolution rate is rising. This is good evidence that widespread testing can have a beneficial effect.
Four days ago the death rate in South Korea was 30%. Today it's just over 10%.
March 14th, 2020:
The next time you hear someone objecting to the "politicization" of the coronavirus response, consider:
The reaction of government and leadership to a pandemic disease is one of, if not the, most political events you will experience.
Everything about the response, from the application of science, math, healthcare, social behavior, individualism-vs-collectivism, capitalism-vs-socialism is inherently political.
What a person believes forms the core of their ideology. That is politics in a nutshell. And right now we are faced with an existential threat that is testing the effectiveness of different political ideologies in countering that threat.
So the next time someone scolds you for criticizing the government's response to the crisis consider this response: "Nature is testing your political beliefs and your ideology and finding them utterly ineffective. I'll continue to call it out so long as people are dying rather than you changing your mind about which way is up."
The next time you hear someone objecting to the "politicization" of the coronavirus response, consider:
The reaction of government and leadership to a pandemic disease is one of, if not the, most political events you will experience.
Everything about the response, from the application of science, math, healthcare, social behavior, individualism-vs-collectivism, capitalism-vs-socialism is inherently political.
What a person believes forms the core of their ideology. That is politics in a nutshell. And right now we are faced with an existential threat that is testing the effectiveness of different political ideologies in countering that threat.
So the next time someone scolds you for criticizing the government's response to the crisis consider this response: "Nature is testing your political beliefs and your ideology and finding them utterly ineffective. I'll continue to call it out so long as people are dying rather than you changing your mind about which way is up."
March 14th, 2020:
This is the daily/hourly maintenance station I set up for Finn and me. You all have something similar in your homes, correct?
This is the daily/hourly maintenance station I set up for Finn and me. You all have something similar in your homes, correct?

March 14th, 2020:
For those of you wanting to get your head around the concept of "exponential growth" and how it relates to the spread of Coronavirus, I wrote something on the subject a decade or so ago:
"Expounding on Exponents"
For those of you wanting to get your head around the concept of "exponential growth" and how it relates to the spread of Coronavirus, I wrote something on the subject a decade or so ago:
"Expounding on Exponents"
March 14th, 2020:
Coronavirus, cold or flu? Here's something that can help you tell which one you or someone else might have:
Coronavirus, cold or flu? Here's something that can help you tell which one you or someone else might have:
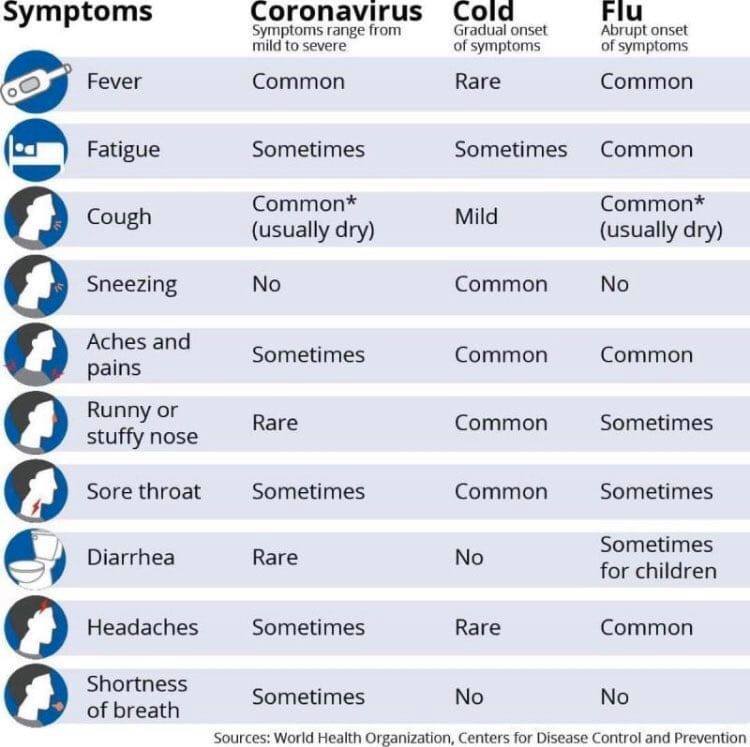
March 14th, 2020:
Since January 22nd of this year to today, the number of coronavirus-infected individuals is increasing by 20% every twenty-four hours. On January 22nd there was 1 official infected. Today there are 2179.
At this rate, by April 30th there will be 9.3 million infected individuals in the United States. This is what that looks like.
At a 2% death rate, that is nearly 200,000 dead by the end of next month.
Since January 22nd of this year to today, the number of coronavirus-infected individuals is increasing by 20% every twenty-four hours. On January 22nd there was 1 official infected. Today there are 2179.
At this rate, by April 30th there will be 9.3 million infected individuals in the United States. This is what that looks like.
At a 2% death rate, that is nearly 200,000 dead by the end of next month.
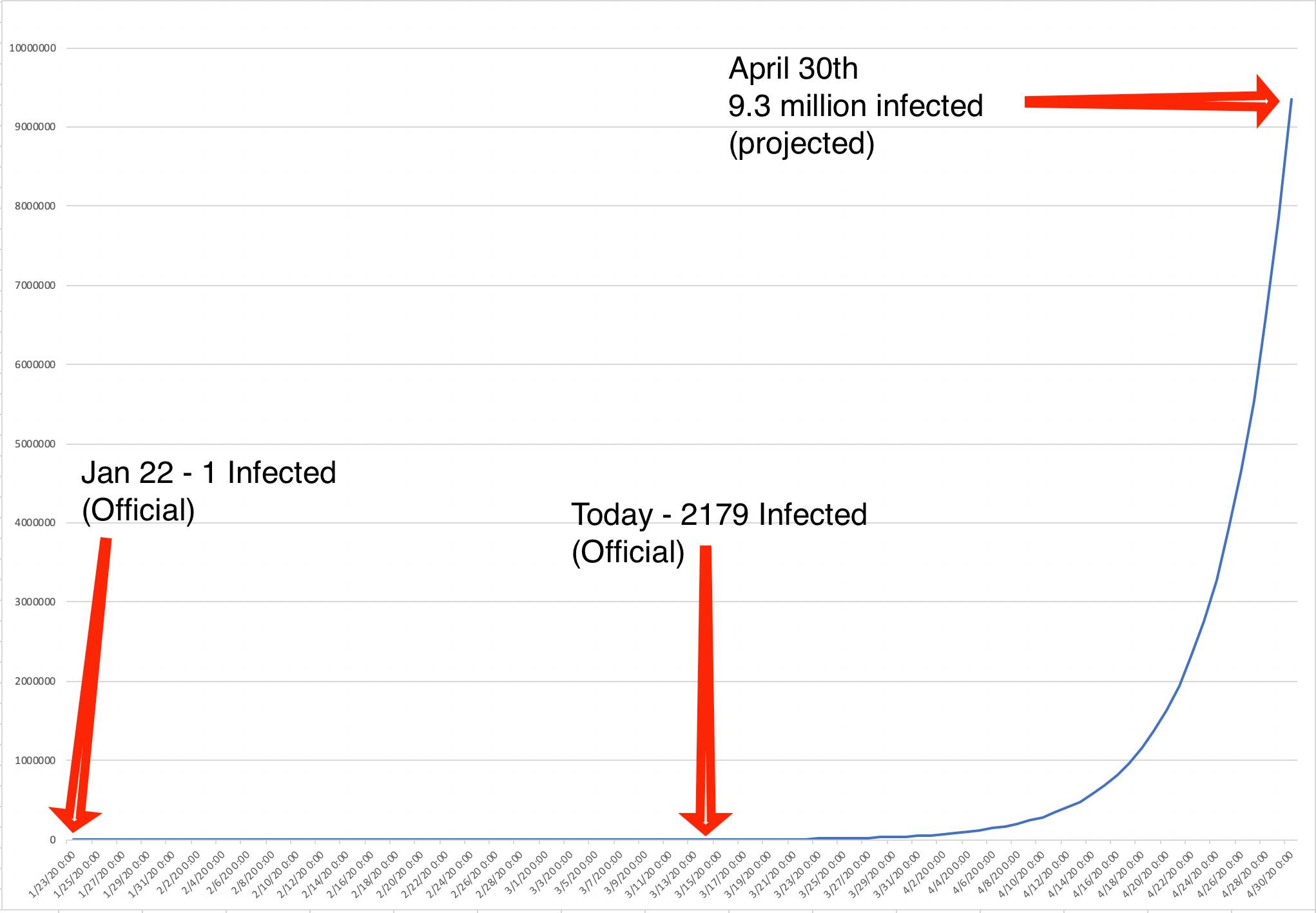
March 14th, 2020:
It's time for some good news:
Within five days, COVID-19 will be eradicated in China. The number of people who either died from it or recovered from it will equal the number of people infected with it.
It's time for some good news:
Within five days, COVID-19 will be eradicated in China. The number of people who either died from it or recovered from it will equal the number of people infected with it.
March 15th, 2020:
This is another excellent set of recommendations. Also includes home made sanitizer recipe!
"How to fight the coronavirus SARS-CoV-2 and its disease, CoVID-19"
This is another excellent set of recommendations. Also includes home made sanitizer recipe!
"How to fight the coronavirus SARS-CoV-2 and its disease, CoVID-19"
March 15th, 2020:
Bill D'Amico asked me "What happens if we get the growth rate down to 5%?"
To recap, earlier this evening I projected that, at current infection growth rates (30%), there will be 14 million infected in the US by mid-April.
What if, through extreme social distancing and lockdowns of certain activities, we can get that down to 5%? What does it look like then?
Assuming we could do that tomorrow (we can't, but we can do it soon -- the Chinese went from a growth rate of 50% on January 25th to less than 1% by February 14th), what do the numbers look like then?
At 5%, starting tomorrow, by mid-April we have only 14,000 -- not 14 million -- infected. Yes, I know that there are already way more than 14,000 infected for real, but I am just going off of a "official" baseline today of about 2500 infected.
This is intended to show just how little change it takes in growth rate to spread things out to a manageable level.
Bill D'Amico asked me "What happens if we get the growth rate down to 5%?"
To recap, earlier this evening I projected that, at current infection growth rates (30%), there will be 14 million infected in the US by mid-April.
What if, through extreme social distancing and lockdowns of certain activities, we can get that down to 5%? What does it look like then?
Assuming we could do that tomorrow (we can't, but we can do it soon -- the Chinese went from a growth rate of 50% on January 25th to less than 1% by February 14th), what do the numbers look like then?
At 5%, starting tomorrow, by mid-April we have only 14,000 -- not 14 million -- infected. Yes, I know that there are already way more than 14,000 infected for real, but I am just going off of a "official" baseline today of about 2500 infected.
This is intended to show just how little change it takes in growth rate to spread things out to a manageable level.
March 15th, 2020:
Good morning! Thought I would start the day with some happy thoughts.
On January 23, China initiated a "lockdown" in Wuhan, enforcing (via drones at times) mandatory "staycations."
On January 23, China had 639 infected and a 16% day-to-day growth rate.
On January 28th, China had 5494 infected and a 90+% growth rate. However, this is the maximum growth rate.
After January 28th, five days after the extreme social distancing, the infection spread began to slow DRAMATICALLY. Within four weeks of the extreme social distancing, it had effectively stopped.
This is doubly-interesting because five days is about the incubation period of SARS-CoV-2 -- i.e. the amount of time between infection and when symptoms start to appear.
The fact that there are only five days between the lockdown date and the date when new infections started to decline sharply indicates that the lockdown took effect IMMEDIATELY.
On February 19th, China had 74,546 infected and a < 1% growth rate. In other words, new infections had virtually stopped by February 19th, less than 4 weeks after the "lockdown."
Good morning! Thought I would start the day with some happy thoughts.
On January 23, China initiated a "lockdown" in Wuhan, enforcing (via drones at times) mandatory "staycations."
On January 23, China had 639 infected and a 16% day-to-day growth rate.
On January 28th, China had 5494 infected and a 90+% growth rate. However, this is the maximum growth rate.
After January 28th, five days after the extreme social distancing, the infection spread began to slow DRAMATICALLY. Within four weeks of the extreme social distancing, it had effectively stopped.
This is doubly-interesting because five days is about the incubation period of SARS-CoV-2 -- i.e. the amount of time between infection and when symptoms start to appear.
The fact that there are only five days between the lockdown date and the date when new infections started to decline sharply indicates that the lockdown took effect IMMEDIATELY.
On February 19th, China had 74,546 infected and a < 1% growth rate. In other words, new infections had virtually stopped by February 19th, less than 4 weeks after the "lockdown."
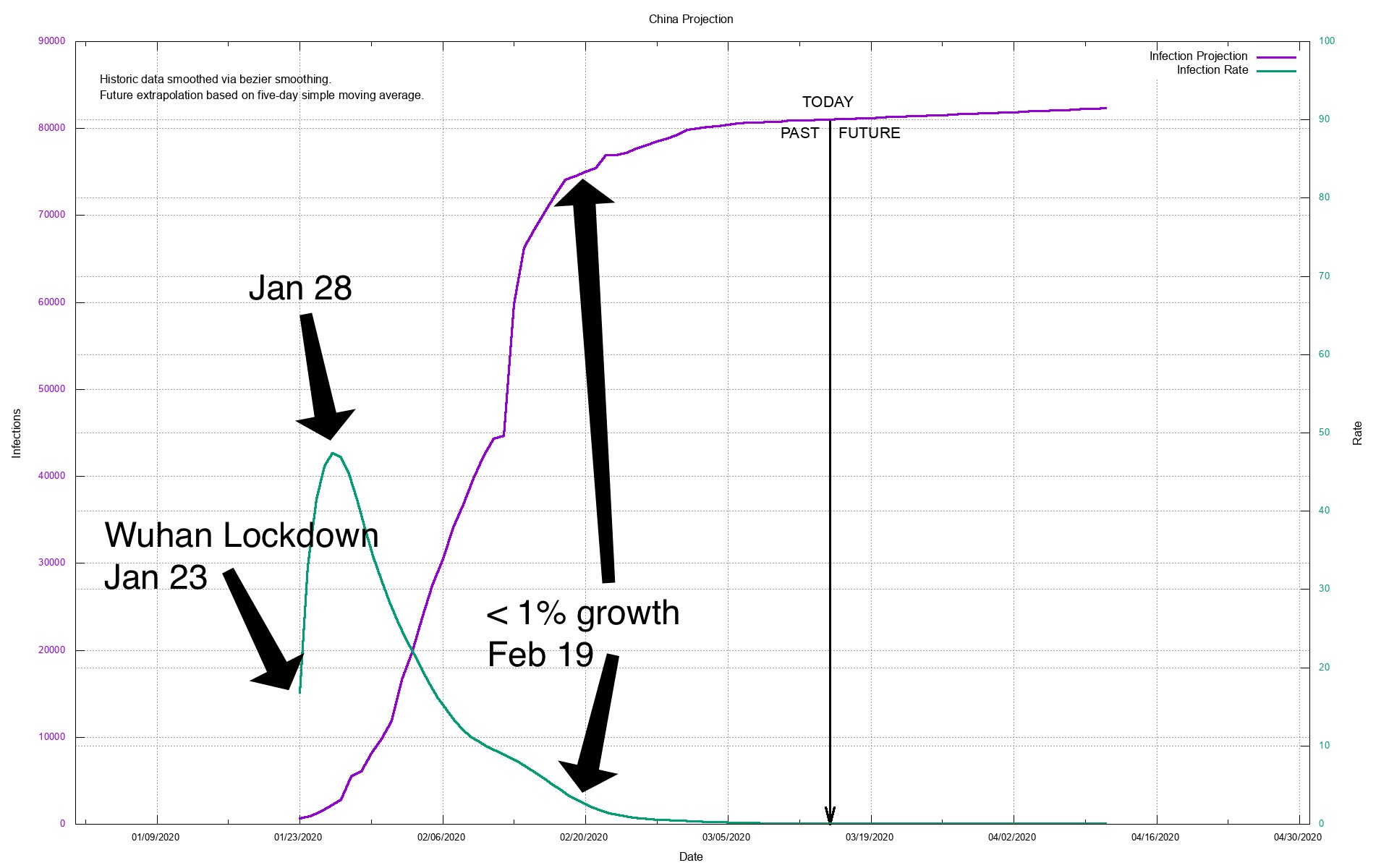
March 15th, 2020:
This is a companion to my last post. It is meant to show where we are headed if we do absolutely nothing. And where we could be with strong social distancing.
We are currently growing the number of infected in the United States at a little over 35% a day, which means that the number of cases doubles every three days or so.
At this rate, we will have over 40 million infected by April 15th (tax day). And 20,000 dead. See first chart here.,
Now if we adopt some strong but reasonable social distancing practices (more to come in my next post) we could get that rate down to 5% fairly quickly. What does 5% look like, compared to 35%?
If we got it down to 5%, we could expect not 40 million infected by tax day but just 13 thousand. And not 20,000 dead but 200. See second chart here.
I think it's worth it, don't you? Now tell your boss.
This is a companion to my last post. It is meant to show where we are headed if we do absolutely nothing. And where we could be with strong social distancing.
We are currently growing the number of infected in the United States at a little over 35% a day, which means that the number of cases doubles every three days or so.
At this rate, we will have over 40 million infected by April 15th (tax day). And 20,000 dead. See first chart here.,
Now if we adopt some strong but reasonable social distancing practices (more to come in my next post) we could get that rate down to 5% fairly quickly. What does 5% look like, compared to 35%?
If we got it down to 5%, we could expect not 40 million infected by tax day but just 13 thousand. And not 20,000 dead but 200. See second chart here.
I think it's worth it, don't you? Now tell your boss.
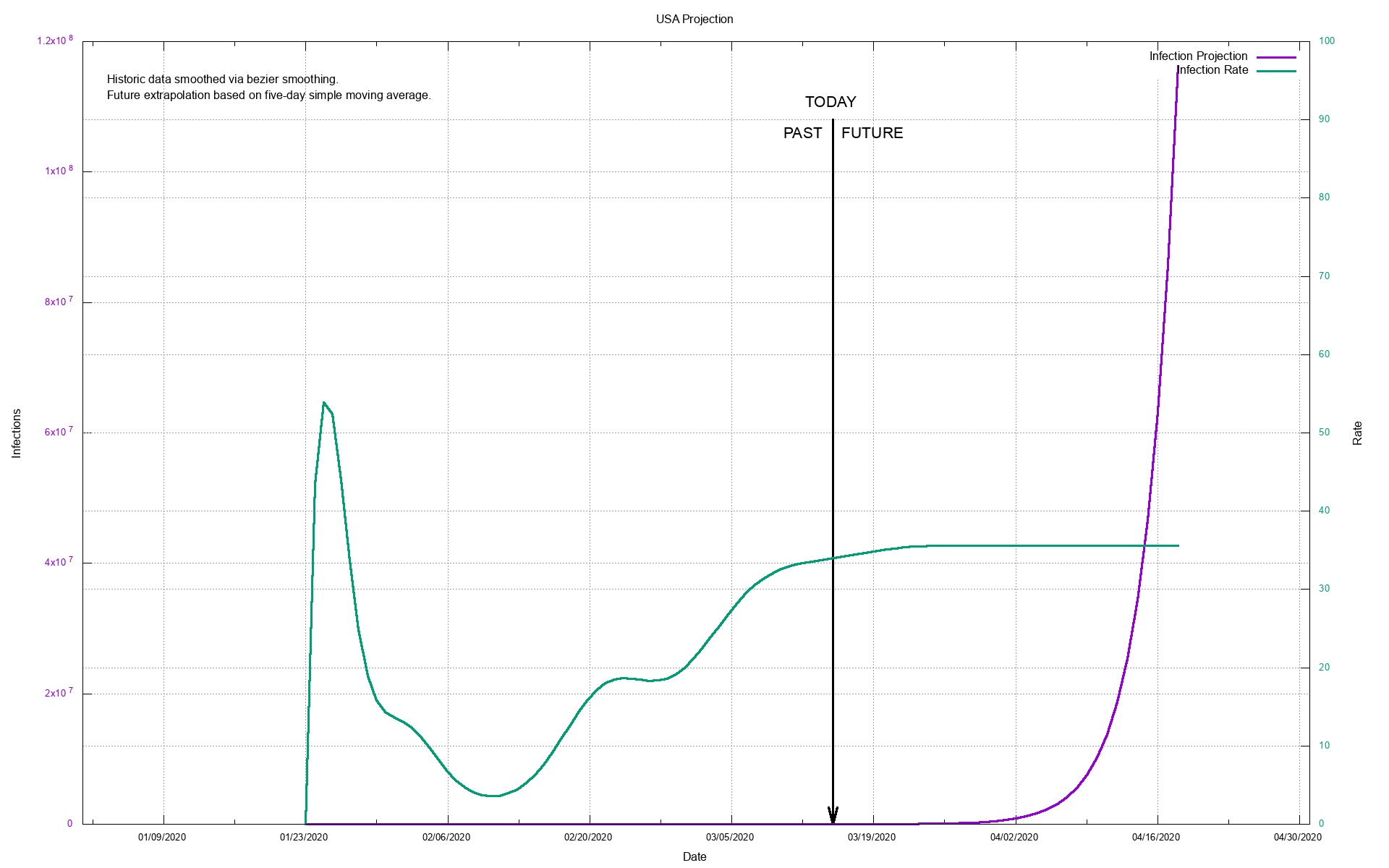
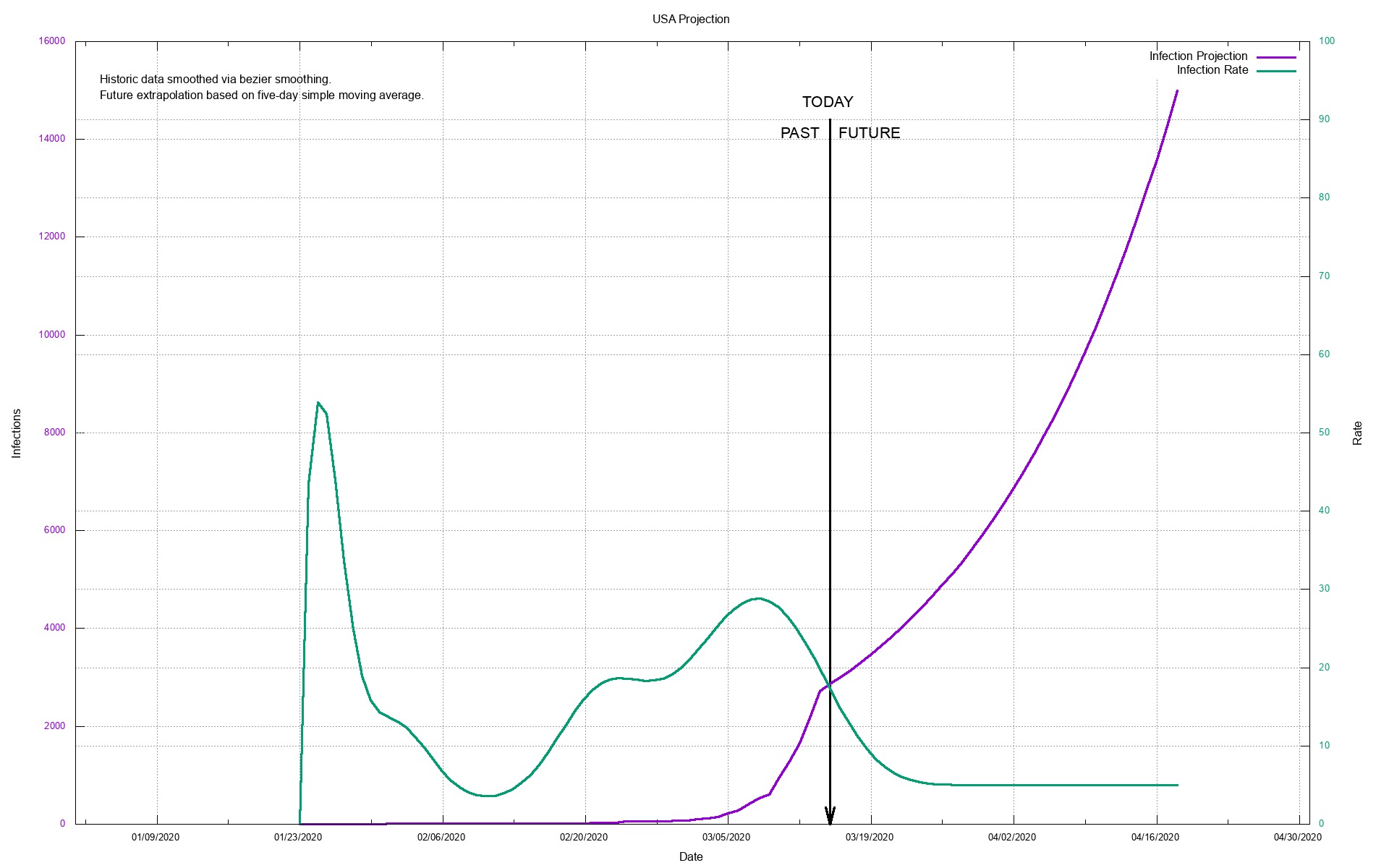
March 15th, 2020:
See my last two posts for background. Here are some prophylactic suggestions for surviving in the age of COVID-19.
First:
COVID-19 - This is the name of the DISEASE that you get from the...
SARS-CoV-2 - Coronavirus. SARS-CoV-2 is the name of the virus.
SARS-CoV-2 is very similar to SARS-CoV-1, which is what we used to just call "SARS." Remember how scary that was? Well, compared to SARS/SARS-CoV-1 (SARS v1), SARS-CoV-2 (SARS v2) is:
a) Less deadly (so far). SARS v1. had a death rate of about 15% (15% of people who got it, died). SARS v2 looks like it is going to have a death rate of about 5% in the US (5% of the people who get it, will die.
b) FAR more easily transmitted. So even though you are less likely to die from SARS v2, far, far, far more people will eventually become infected. I expect the global infection rate to eventually match that of the Influenza pandemic of 1918, i.e. about half of us will contract it. And that means that it is going to kill far more people than SARS v1 did.
Now the good news is that because the current SARS is so similar to the original SARS, a lot of the research done on original-recipe SARS (v1) is applicable to extra-crispy SARS (v2). Including supportive medications (anti-virals) and vaccinations. A vaccine for SARS v1 was not available until after the epidemic was over. It is likely that we could develop a vaccine for SARS v2 fairly rapidly, though I do not want to generate false hope.
How COVID-19 kills you:
a) It infects your lungs and compromises their ability to take the oxygen in the air out of the air and put it into your bloodstream. It does this by converting nice, wet, squishy lung tissue into hard fibrous tissue. I believe the fibrous process is amyloid. This is similar to the process that killed my late wife, Sophia, although in her case it was not a virus but her own immune system that deposited amyloid proteins in her heart muscle.
Easiest way to visualize it is your lungs get stiff and dry and full of what is a kissing-cousin to scab material.
[NOTE: Not quite sure this is perfectly accurate]
b) Your compromised lungs and immune system then are further insulted by bacteria. That turns into pneumonia which causes the remaining capacity of your lungs to go to zero.
c) You suffocate and die.
This is why ventilators are so important -- they increase your lungs' ability to take oxygen out by first artificially inflating them (remember they are hard and stiff now) and second forcing oxygen into them.
There is another set of machinery that can introduce oxygen directly into the bloodstream. However that machinery is extremely scare.
[NOTE: Lots of information that actual mechanism of death may be cardiac arrest]
Third prophylactic post:
The last thing you want to do, under any circumstances, is visit your doctor, and ER, or a hospital at this point. So a lot of your effort should be concentrated on making sure you do not visit one. Why?
Because a) You do not want to add to the burden of the health care industry if it's not necessary and
b) If you don't have COVID-19 and you visit a hospital, ER or even your doctor's office, you will have it when your visit is over.
Ok, so how can you determine, at home, if you have contracted COVID-19?
a). Has it been more than 10 days since you had social contact with anyone? Are you symptom free? You do not have it.
b) If the answer to a) is "no." Then: 1) Do you have a fever over 100? If "yes" then: 2) Is your nose dry (not runny) and are you not sneezing? If "yes" then 3) Do you have a dry cough? If "yes" then try and take your blood oxygen level (you can get testers for about $30 on Amazon (maybe)). Less than 92%?
Congratulations, you might have COVID-19. Call your doctor.
How will I get it?
You will contract COVID-19 primarily from two vectors:
1. Someone with COVID-19 will sneeze or cough within six-10 feet of you and you will inhale the virus.
2. Someone with COVID-19 will touch something that you then touch.
Who are these "someones?" They are primarily young people in the 0-30 age demographic who are early in their infection. They were exposed to the virus themselves 2-5 days before they exposed you to it. Virus counts appear to be highest in the two days BEFORE symptoms appear, i.e. we are most contagious JUST BEFORE they start feeling bad. All young people in the 0-30 age group who are two to zero+plus+2 days of being symptomatic should be considered "superspreaders." each one capable of infecting many more.
Others are just mere spreaders.
Stay away from people, particularly young people who have not yet begun to responsibly self-quarantine/engage in social distancing. I am seeing terrifying pictures of packed bars in New York full of young people, choked streets in the French Quarter of New Orleans, etc. All of those people are now infected. Stay away from them.
Second, stay away from likely places of high contamination. The most dirty place in the world is a hospital ER. The second most dirty place in the world is the waiting room at your pediatrician. The third is the waiting room at your doctor's office. The close runner-up is your dentist.
Following that are ANY social gatherings, particularly birthday parties for young children, buffets, mass transit. Virtually anywhere where there are many people and who are not maintaining strict hygiene and physical separation. It just takes one person with the virus in a group to infect most of the group. Boston was contaminated completely because one or two people at a < 100 person conference contracted COVID-19 (and were pre-symptoms) and shared the same serving utensils at at collective lunch buffet with uninfected people.
What should you do?
1. Consider everything you come in contact with to be contaminated with SARS-CoV-2 unless you have a good reason to believe it is not. These things include:
a) Anything someone hands to you. Think drive-through services (food, banking, etc.) but really, anything.
b) Anything someone else touches. Elevator buttons. Supermarket self-checkout screens. Handrails. Furniture. Etc.
You cannot avoid touching things that other people have touched. But you can practice decontamination when you do. If you touch something that you are not reasonably sure is clean DO NOT TOUCH YOUR OWN FACE UNTIL YOU HAVE DECONTAMINATED (washed) YOUR HANDS. Moreover, ANYTHING you touch between the time you touched something else and you wash your hands needs to also be decontaminated.
Once you are reasonably certain that your environment is safe, then it is perfectly OK to touch your face with your own hands. So if someone comes to visit a) Keep your distance and b) Decontaminate once they leave, being sure to decontaminate all surfaces they may have touched (windex works well for this. If you don't care about your furniture, you can use clorox+water spray also). Pay particular attention to doorknobs, particularly if they are metal. The virus does not live long on paper or cardboard but it can live up to 3-5 days on hard plastic and metal.
2. We're not all bozos on this bus. Most of us will be very responsible, not only for our own health but for the health of others. Unfortunately a few will be extremely irresponsible. Avoid them like the plague, because that's exactly what they are. Warning signs:
a) Goes to social gatherings, restaurants, parties, bars, etc. as if there was nothing going on.
b) Says things like "It's just like the flu" (it is not) or "Most people won't even notice they have it" (they will).
Men: Do not be that kind of asshole. Women: Do not fuck those assholes. Protect yourselves and send a message at the same time.
See my last two posts for background. Here are some prophylactic suggestions for surviving in the age of COVID-19.
First:
COVID-19 - This is the name of the DISEASE that you get from the...
SARS-CoV-2 - Coronavirus. SARS-CoV-2 is the name of the virus.
SARS-CoV-2 is very similar to SARS-CoV-1, which is what we used to just call "SARS." Remember how scary that was? Well, compared to SARS/SARS-CoV-1 (SARS v1), SARS-CoV-2 (SARS v2) is:
a) Less deadly (so far). SARS v1. had a death rate of about 15% (15% of people who got it, died). SARS v2 looks like it is going to have a death rate of about 5% in the US (5% of the people who get it, will die.
b) FAR more easily transmitted. So even though you are less likely to die from SARS v2, far, far, far more people will eventually become infected. I expect the global infection rate to eventually match that of the Influenza pandemic of 1918, i.e. about half of us will contract it. And that means that it is going to kill far more people than SARS v1 did.
Now the good news is that because the current SARS is so similar to the original SARS, a lot of the research done on original-recipe SARS (v1) is applicable to extra-crispy SARS (v2). Including supportive medications (anti-virals) and vaccinations. A vaccine for SARS v1 was not available until after the epidemic was over. It is likely that we could develop a vaccine for SARS v2 fairly rapidly, though I do not want to generate false hope.
How COVID-19 kills you:
a) It infects your lungs and compromises their ability to take the oxygen in the air out of the air and put it into your bloodstream. It does this by converting nice, wet, squishy lung tissue into hard fibrous tissue. I believe the fibrous process is amyloid. This is similar to the process that killed my late wife, Sophia, although in her case it was not a virus but her own immune system that deposited amyloid proteins in her heart muscle.
Easiest way to visualize it is your lungs get stiff and dry and full of what is a kissing-cousin to scab material.
[NOTE: Not quite sure this is perfectly accurate]
b) Your compromised lungs and immune system then are further insulted by bacteria. That turns into pneumonia which causes the remaining capacity of your lungs to go to zero.
c) You suffocate and die.
This is why ventilators are so important -- they increase your lungs' ability to take oxygen out by first artificially inflating them (remember they are hard and stiff now) and second forcing oxygen into them.
There is another set of machinery that can introduce oxygen directly into the bloodstream. However that machinery is extremely scare.
[NOTE: Lots of information that actual mechanism of death may be cardiac arrest]
Third prophylactic post:
The last thing you want to do, under any circumstances, is visit your doctor, and ER, or a hospital at this point. So a lot of your effort should be concentrated on making sure you do not visit one. Why?
Because a) You do not want to add to the burden of the health care industry if it's not necessary and
b) If you don't have COVID-19 and you visit a hospital, ER or even your doctor's office, you will have it when your visit is over.
Ok, so how can you determine, at home, if you have contracted COVID-19?
a). Has it been more than 10 days since you had social contact with anyone? Are you symptom free? You do not have it.
b) If the answer to a) is "no." Then: 1) Do you have a fever over 100? If "yes" then: 2) Is your nose dry (not runny) and are you not sneezing? If "yes" then 3) Do you have a dry cough? If "yes" then try and take your blood oxygen level (you can get testers for about $30 on Amazon (maybe)). Less than 92%?
Congratulations, you might have COVID-19. Call your doctor.
How will I get it?
You will contract COVID-19 primarily from two vectors:
1. Someone with COVID-19 will sneeze or cough within six-10 feet of you and you will inhale the virus.
2. Someone with COVID-19 will touch something that you then touch.
Who are these "someones?" They are primarily young people in the 0-30 age demographic who are early in their infection. They were exposed to the virus themselves 2-5 days before they exposed you to it. Virus counts appear to be highest in the two days BEFORE symptoms appear, i.e. we are most contagious JUST BEFORE they start feeling bad. All young people in the 0-30 age group who are two to zero+plus+2 days of being symptomatic should be considered "superspreaders." each one capable of infecting many more.
Others are just mere spreaders.
Stay away from people, particularly young people who have not yet begun to responsibly self-quarantine/engage in social distancing. I am seeing terrifying pictures of packed bars in New York full of young people, choked streets in the French Quarter of New Orleans, etc. All of those people are now infected. Stay away from them.
Second, stay away from likely places of high contamination. The most dirty place in the world is a hospital ER. The second most dirty place in the world is the waiting room at your pediatrician. The third is the waiting room at your doctor's office. The close runner-up is your dentist.
Following that are ANY social gatherings, particularly birthday parties for young children, buffets, mass transit. Virtually anywhere where there are many people and who are not maintaining strict hygiene and physical separation. It just takes one person with the virus in a group to infect most of the group. Boston was contaminated completely because one or two people at a < 100 person conference contracted COVID-19 (and were pre-symptoms) and shared the same serving utensils at at collective lunch buffet with uninfected people.
What should you do?
1. Consider everything you come in contact with to be contaminated with SARS-CoV-2 unless you have a good reason to believe it is not. These things include:
a) Anything someone hands to you. Think drive-through services (food, banking, etc.) but really, anything.
b) Anything someone else touches. Elevator buttons. Supermarket self-checkout screens. Handrails. Furniture. Etc.
You cannot avoid touching things that other people have touched. But you can practice decontamination when you do. If you touch something that you are not reasonably sure is clean DO NOT TOUCH YOUR OWN FACE UNTIL YOU HAVE DECONTAMINATED (washed) YOUR HANDS. Moreover, ANYTHING you touch between the time you touched something else and you wash your hands needs to also be decontaminated.
Once you are reasonably certain that your environment is safe, then it is perfectly OK to touch your face with your own hands. So if someone comes to visit a) Keep your distance and b) Decontaminate once they leave, being sure to decontaminate all surfaces they may have touched (windex works well for this. If you don't care about your furniture, you can use clorox+water spray also). Pay particular attention to doorknobs, particularly if they are metal. The virus does not live long on paper or cardboard but it can live up to 3-5 days on hard plastic and metal.
2. We're not all bozos on this bus. Most of us will be very responsible, not only for our own health but for the health of others. Unfortunately a few will be extremely irresponsible. Avoid them like the plague, because that's exactly what they are. Warning signs:
a) Goes to social gatherings, restaurants, parties, bars, etc. as if there was nothing going on.
b) Says things like "It's just like the flu" (it is not) or "Most people won't even notice they have it" (they will).
Men: Do not be that kind of asshole. Women: Do not fuck those assholes. Protect yourselves and send a message at the same time.
March 15th, 2020:
Oh, one more thing. If you have any kind of periodic visits to your home by a professional service, now is the time to stop it.
For example, I have maid service that comes to my house. I am going to tell them not to come next week -- for their protection and mine.
However, and this is very important, I am still going to pay them as if they did come.
Everyone, every business, has a self-interest in making sure that those on whom they depend (i.e. their employees) are still going to be there for them when we come out the other side of this.
Oh, one more thing. If you have any kind of periodic visits to your home by a professional service, now is the time to stop it.
For example, I have maid service that comes to my house. I am going to tell them not to come next week -- for their protection and mine.
However, and this is very important, I am still going to pay them as if they did come.
Everyone, every business, has a self-interest in making sure that those on whom they depend (i.e. their employees) are still going to be there for them when we come out the other side of this.
March 15th, 2020:
There is someone on MSNBC (Michael Osterholm) right now saying that there is no evidence that closing schools is helpful.
It was/is my understanding that we had a lot of empirical evidence to the exact opposite.
Reading his past statements on the matter, he appears to be taking that position on a belief that children cannot be infected. He seems to base that on the lower incidence of disease/symptoms in children.
It is my understanding that children are equally able to contract the disease, they just don't react (in general) as badly as older people. That means they can be carriers as easily as anyone, they just don't get sick.
There is someone on MSNBC (Michael Osterholm) right now saying that there is no evidence that closing schools is helpful.
It was/is my understanding that we had a lot of empirical evidence to the exact opposite.
Reading his past statements on the matter, he appears to be taking that position on a belief that children cannot be infected. He seems to base that on the lower incidence of disease/symptoms in children.
It is my understanding that children are equally able to contract the disease, they just don't react (in general) as badly as older people. That means they can be carriers as easily as anyone, they just don't get sick.
March 15th, 2020:
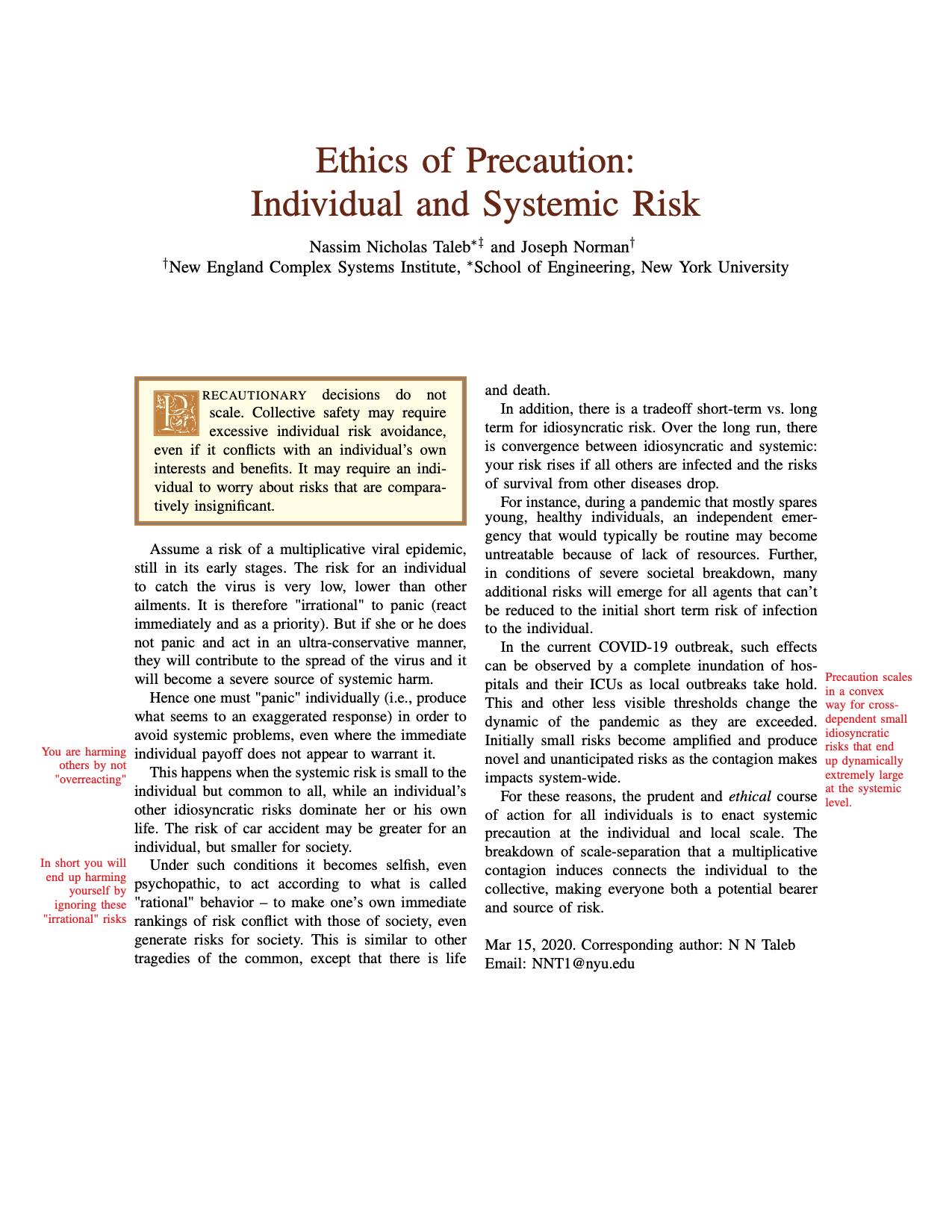
March 15th, 2020:
On the ground in Seattle. This was sent to me. I am not the friend of the nurse who wrote this:
"From a nurse friend of mine in Seattle For my CCU friends... This is from a front-line ICU physician in a Seattle hospital
This is his personal account:
* we have 21 pts and 11 deaths since 2/28.
* we are seeing pts who are young (20s), fit, no comorbidities, critically ill. It does happen.
* US has been past containment since January
* Currently, all of ICU is for critically ill COVIDs, all of floor medsurg for stable COVIDs and EOL care, half of PCU, half of ER. New resp-sx pts Pulmonary Clinic offshoot is open
* CDC is no longer imposing home quarantine on providers who were wearing only droplet iso PPE when intubating, suctioning, bronching, and in one case doing bloody neurosurgery. Expect when it comes to your place you may initially have staff home-quarantined. Plan for this NOW. Consider wearing airborne iso PPE for aerosol-generating procedures in ANY pt in whom you suspect COVID, just to prevent the mass quarantines.
* we ran out of N95s (thanks, Costco hoarders) and are bleaching and re-using PAPRs, which is not the manufacturer's recommendation. Not surprised on N95s as we use mostly CAPRs anyway, but still.
*terminal cleans (inc UV light) for ER COVID rooms are taking forever, Enviro Services is overwhelmed. Bad as pts are stuck coughing in the waiting room. Rec planning now for Enviro upstaffing, or having a plan for sick pts to wait in their cars (that is not legal here, sadly).
* CLINICAL INFO based on our cases and info from CDC conf call today with other COVID providers in US:
* the Chinese data on 80% mildly ill, 14% hospital-ill, 6-8% critically ill are generally on the mark. Data very skewed by late and very limited testing, and the number of our elderly pts going to comfort care. - being young & healthy (zero medical problems) does not rule out becoming vented or dead - probably the time course to developing significant lower resp sx is about a week or longer (which also fits with timing of sick cases we started seeing here, after we all assumed it was endemic as of late Jan/early Feb). - based on our hospitalized cases (including the not formally diagnosed ones who are obviously COVID - it is quite clinically unique) about 1/3 have mild lower resp sx, need 1-5L NC. 1/3 are sicker, FM or NRB. 1/3 tubed with ARDS. Thus far, everyone is seeing: - nl WBC. Almost always lymphopenic, occasionally poly-predominant but with nl total WBC. Doesn't change, even 10days in. - BAL lymphocytic despite blood lymphopenic (try not to bronch these pts; this data is from pre-testing time when we had several idiopathic ARDS cases) - fevers, often high, may be intermittent; persistently febrile, often for >10d. It isn't the dexmed, it's the SARS2. - low ProCalc; may be useful to check initially for later trending if later concern for VAP etc. - up AST/ALT, sometimes alk phos. Usually in 70-100 range. No fulminant hepatitis. Notably, in our small sample, higher transaminitis at admit (150-200) correlates with clinical deterioration and progression to ARDS. LFTs typically begin to bump in 2nd week of clinical course. - mild AKI (Cr <2). Uncertain if direct viral effect, but notably SARS2 RNA fragments have been identified in liver, kidneys, heart, and blood.
* characteristic CXR always bilateral patchy or reticular infiltrates, sometimes perihilar despite nl EF and volume down at presentation. At time of presentation may be subtle, but always present, even in our pts on chronic high dose steroids. NO effusions. CT is as expected, rarely mild mediastinal LAD, occ small effusions late in course which might be related to volume status/cap leak.
* Note - China is CT'ing everyone, even outpts, as a primarily diagnostic modality. However, in US/Europe, CT is rare, since findings are nonspecific, would not change management, and the ENTIRE scanner and room have to terminal-cleaned, which is just impossible in a busy hospital. Also, transport in PAPRs. Etc. 2 of our pts had CTs for idiopathic ARDS in the pre-test era; they looked like the CTs in the journal articles. Not more helpful than CXR. - when resp failure occurs, it is RAPID (likely 7-10d out from sx onset, but rapid progression from hospital admit). Common scenario for our pts is, admit 1L NC. Next 12hrs -> NPPV. Next 12-24hrs -> vent/proned/Flolan. - interestingly, despite some needing Flolan, the hypoxia is not as refractory as with H1N1. Quite different, and quite unique. Odd enough that you'd notice and say hmmm. - thus far many are dying of cardiac arrest rather than inability to ventilate/oxygenate. - given the inevitable rapid progression to ETT once resp decompensation begins, we and other hosps, including Wuhan, are doing early intubation. Facemask is fine, but if needing HFNC or NPPV just tube them. They definitely will need a tube anyway, & no point risking the aerosols. - no MOSF. There's the mild AST/ALT elevation, maybe a small Cr bump, but no florid failure. except cardiomyopathy. - multiple pts here have had nl EF on formal Echo or POCUS at time of admit (or in a couple of cases EF 40ish, chronically). Also nl Tpn from ED. Then they get the horrible resp failure, sans sepsis or shock. Then they turn the corner, off Flolan, supined, vent weaning, looking good, never any pressor requirement. Then over 12hrs, newly cold, clamped, multiple-pressor shock that looks cardiogenic, EF 10% or less, then either VT->VF-> dead or PEA-> asystole in less than a day. Needless to say this is awful for families who had started to have hope. - We have actually had more asystole than VT, other facilities report more VT/VF, but same time course, a few days or a week after admit, around the time they're turning the corner. This occurs on med-surg pts too; one today who is elderly and chronically ill but baseline EF preserved, newly hypoTN overnight, EF<10. Already no escalation, has since passed, So presumably there is a viral CM aspect, which presents later in the course of dz. - of note, no WMAs on Echo, RV preserved, Tpns don't bump. Could be unrelated, but I've never seen anything like it before, esp in a pt who had been HD stable without sepsis.
Treatment -
*Remdesivir might work, some hosps have seen improvement with it quite rapidly, marked improvement in 1-3 days. ARDS trajectory is impressive with it, pts improve much more rapidly than expected in usual ARDS.
*Recommended course is 10d, but due to scarcity all hosps have stopped it when pt clinically out of the woods - none have continued >5d. It might cause LFT bump, but interestingly seem to bump (200s-ish) for a day or 2 after starting then rapidly back to normal - suggests not a primary toxic hepatitis.
*unfortunately, the Gilead compassionate use and trial programs require AST/ALT <5x normal, which is pretty much almost no actual COVID pts. Also CrCl>30, which is fine. CDC is working with Gilead to get LFT reqs changed now that we know this is a mild viral hepatitis.
-currently the Gilead trial is wrapping up, NIH trial still enrolling, some new trial soon to begin can't remember where.
*steroids are up in the air. In China usual clinical practice for all ARDS is high dose methylpred. Thus, ALL of their pts have had high dose methylpred. Some question whether this practice increases mortality.
*it is likely that it increases seconday VAP/HAP. China has had a high rate of drug resistant GNR HAP/VAP and fungal pna in these pts, with resulting increases mortality. We have seen none, even in the earlier pts who were vented for >10d before being bronched (prior to test availability, again it is not a great idea to bronch these pts now).
- unclear whether VAP-prevention strategies are also different, but wouldn't think so?
- Hong Kong is currently running an uncontrolled trial of HC 100IV Q8.
- general consensus here (in US among docs who have cared for COVID pts) is that steroids will do more harm than good, unless needed for other indications.
- many of our pts have COPD on ICS. Current consensus at Evergreen, after some observation & some clinical judgment, is to stop ICS if able, based on known data with other viral pneumonias and increased susceptibility to HAP. Thus far pts are tolerating that, no major issues with ventilating them that can't be managed with vent changes. We also have quite a few on AE-COPD/asthma doses of methylpred, so will be interesting to see how they do.
Plz share info."
On the ground in Seattle. This was sent to me. I am not the friend of the nurse who wrote this:
"From a nurse friend of mine in Seattle For my CCU friends... This is from a front-line ICU physician in a Seattle hospital
This is his personal account:
* we have 21 pts and 11 deaths since 2/28.
* we are seeing pts who are young (20s), fit, no comorbidities, critically ill. It does happen.
* US has been past containment since January
* Currently, all of ICU is for critically ill COVIDs, all of floor medsurg for stable COVIDs and EOL care, half of PCU, half of ER. New resp-sx pts Pulmonary Clinic offshoot is open
* CDC is no longer imposing home quarantine on providers who were wearing only droplet iso PPE when intubating, suctioning, bronching, and in one case doing bloody neurosurgery. Expect when it comes to your place you may initially have staff home-quarantined. Plan for this NOW. Consider wearing airborne iso PPE for aerosol-generating procedures in ANY pt in whom you suspect COVID, just to prevent the mass quarantines.
* we ran out of N95s (thanks, Costco hoarders) and are bleaching and re-using PAPRs, which is not the manufacturer's recommendation. Not surprised on N95s as we use mostly CAPRs anyway, but still.
*terminal cleans (inc UV light) for ER COVID rooms are taking forever, Enviro Services is overwhelmed. Bad as pts are stuck coughing in the waiting room. Rec planning now for Enviro upstaffing, or having a plan for sick pts to wait in their cars (that is not legal here, sadly).
* CLINICAL INFO based on our cases and info from CDC conf call today with other COVID providers in US:
* the Chinese data on 80% mildly ill, 14% hospital-ill, 6-8% critically ill are generally on the mark. Data very skewed by late and very limited testing, and the number of our elderly pts going to comfort care. - being young & healthy (zero medical problems) does not rule out becoming vented or dead - probably the time course to developing significant lower resp sx is about a week or longer (which also fits with timing of sick cases we started seeing here, after we all assumed it was endemic as of late Jan/early Feb). - based on our hospitalized cases (including the not formally diagnosed ones who are obviously COVID - it is quite clinically unique) about 1/3 have mild lower resp sx, need 1-5L NC. 1/3 are sicker, FM or NRB. 1/3 tubed with ARDS. Thus far, everyone is seeing: - nl WBC. Almost always lymphopenic, occasionally poly-predominant but with nl total WBC. Doesn't change, even 10days in. - BAL lymphocytic despite blood lymphopenic (try not to bronch these pts; this data is from pre-testing time when we had several idiopathic ARDS cases) - fevers, often high, may be intermittent; persistently febrile, often for >10d. It isn't the dexmed, it's the SARS2. - low ProCalc; may be useful to check initially for later trending if later concern for VAP etc. - up AST/ALT, sometimes alk phos. Usually in 70-100 range. No fulminant hepatitis. Notably, in our small sample, higher transaminitis at admit (150-200) correlates with clinical deterioration and progression to ARDS. LFTs typically begin to bump in 2nd week of clinical course. - mild AKI (Cr <2). Uncertain if direct viral effect, but notably SARS2 RNA fragments have been identified in liver, kidneys, heart, and blood.
* characteristic CXR always bilateral patchy or reticular infiltrates, sometimes perihilar despite nl EF and volume down at presentation. At time of presentation may be subtle, but always present, even in our pts on chronic high dose steroids. NO effusions. CT is as expected, rarely mild mediastinal LAD, occ small effusions late in course which might be related to volume status/cap leak.
* Note - China is CT'ing everyone, even outpts, as a primarily diagnostic modality. However, in US/Europe, CT is rare, since findings are nonspecific, would not change management, and the ENTIRE scanner and room have to terminal-cleaned, which is just impossible in a busy hospital. Also, transport in PAPRs. Etc. 2 of our pts had CTs for idiopathic ARDS in the pre-test era; they looked like the CTs in the journal articles. Not more helpful than CXR. - when resp failure occurs, it is RAPID (likely 7-10d out from sx onset, but rapid progression from hospital admit). Common scenario for our pts is, admit 1L NC. Next 12hrs -> NPPV. Next 12-24hrs -> vent/proned/Flolan. - interestingly, despite some needing Flolan, the hypoxia is not as refractory as with H1N1. Quite different, and quite unique. Odd enough that you'd notice and say hmmm. - thus far many are dying of cardiac arrest rather than inability to ventilate/oxygenate. - given the inevitable rapid progression to ETT once resp decompensation begins, we and other hosps, including Wuhan, are doing early intubation. Facemask is fine, but if needing HFNC or NPPV just tube them. They definitely will need a tube anyway, & no point risking the aerosols. - no MOSF. There's the mild AST/ALT elevation, maybe a small Cr bump, but no florid failure. except cardiomyopathy. - multiple pts here have had nl EF on formal Echo or POCUS at time of admit (or in a couple of cases EF 40ish, chronically). Also nl Tpn from ED. Then they get the horrible resp failure, sans sepsis or shock. Then they turn the corner, off Flolan, supined, vent weaning, looking good, never any pressor requirement. Then over 12hrs, newly cold, clamped, multiple-pressor shock that looks cardiogenic, EF 10% or less, then either VT->VF-> dead or PEA-> asystole in less than a day. Needless to say this is awful for families who had started to have hope. - We have actually had more asystole than VT, other facilities report more VT/VF, but same time course, a few days or a week after admit, around the time they're turning the corner. This occurs on med-surg pts too; one today who is elderly and chronically ill but baseline EF preserved, newly hypoTN overnight, EF<10. Already no escalation, has since passed, So presumably there is a viral CM aspect, which presents later in the course of dz. - of note, no WMAs on Echo, RV preserved, Tpns don't bump. Could be unrelated, but I've never seen anything like it before, esp in a pt who had been HD stable without sepsis.
Treatment -
*Remdesivir might work, some hosps have seen improvement with it quite rapidly, marked improvement in 1-3 days. ARDS trajectory is impressive with it, pts improve much more rapidly than expected in usual ARDS.
*Recommended course is 10d, but due to scarcity all hosps have stopped it when pt clinically out of the woods - none have continued >5d. It might cause LFT bump, but interestingly seem to bump (200s-ish) for a day or 2 after starting then rapidly back to normal - suggests not a primary toxic hepatitis.
*unfortunately, the Gilead compassionate use and trial programs require AST/ALT <5x normal, which is pretty much almost no actual COVID pts. Also CrCl>30, which is fine. CDC is working with Gilead to get LFT reqs changed now that we know this is a mild viral hepatitis.
-currently the Gilead trial is wrapping up, NIH trial still enrolling, some new trial soon to begin can't remember where.
*steroids are up in the air. In China usual clinical practice for all ARDS is high dose methylpred. Thus, ALL of their pts have had high dose methylpred. Some question whether this practice increases mortality.
*it is likely that it increases seconday VAP/HAP. China has had a high rate of drug resistant GNR HAP/VAP and fungal pna in these pts, with resulting increases mortality. We have seen none, even in the earlier pts who were vented for >10d before being bronched (prior to test availability, again it is not a great idea to bronch these pts now).
- unclear whether VAP-prevention strategies are also different, but wouldn't think so?
- Hong Kong is currently running an uncontrolled trial of HC 100IV Q8.
- general consensus here (in US among docs who have cared for COVID pts) is that steroids will do more harm than good, unless needed for other indications.
- many of our pts have COPD on ICS. Current consensus at Evergreen, after some observation & some clinical judgment, is to stop ICS if able, based on known data with other viral pneumonias and increased susceptibility to HAP. Thus far pts are tolerating that, no major issues with ventilating them that can't be managed with vent changes. We also have quite a few on AE-COPD/asthma doses of methylpred, so will be interesting to see how they do.
Plz share info."
March 15th, 2020:
Statement from the Rector of the Norwegian University of Science and Technology (h/t Mike Conley )
"In line with the advice from the Ministry of Foreign Affairs, I, as NTNU’s Rector, strongly recommend that all NTNU students who are outside Norway return home.
This applies especially if you are staying in a country with poorly developed health services. This also applies for countries with poorly developed collective infrastructure, for example the USA, where it can be difficult to get transport to the airport if you don't have a car. The same applies if you don't have health insurance. "
He's talking about us.
Statement from the Rector of the Norwegian University of Science and Technology (h/t Mike Conley )
"In line with the advice from the Ministry of Foreign Affairs, I, as NTNU’s Rector, strongly recommend that all NTNU students who are outside Norway return home.
This applies especially if you are staying in a country with poorly developed health services. This also applies for countries with poorly developed collective infrastructure, for example the USA, where it can be difficult to get transport to the airport if you don't have a car. The same applies if you don't have health insurance. "
He's talking about us.
March 15th, 2020:
Latest data, just came out. For the United States, if current rates of exponential increase continue:
Forty days from now (April 24th), current rates suggest:
111 million infected by April 24th
42 thousand dead 343 recovered 110 million sick, 30 million critically sick
In a couple weeks the data for the US should settle down -- in particular I would expect the recovery rate to increase and that death rate to decrease so we may be looking at a few thousand recovered in 40 days an a few thousand less deaths than 42 thousand
Latest data, just came out. For the United States, if current rates of exponential increase continue:
Forty days from now (April 24th), current rates suggest:
111 million infected by April 24th
42 thousand dead 343 recovered 110 million sick, 30 million critically sick
In a couple weeks the data for the US should settle down -- in particular I would expect the recovery rate to increase and that death rate to decrease so we may be looking at a few thousand recovered in 40 days an a few thousand less deaths than 42 thousand
March 15th, 2020:
Texted this to Finn's nanny, Ruth, from a hotel room in Madison, Wisconsin on January 28th, 2020 (I had flown to Wisconsin for a dog rescue (Cody))
Texted this to Finn's nanny, Ruth, from a hotel room in Madison, Wisconsin on January 28th, 2020 (I had flown to Wisconsin for a dog rescue (Cody))

March 16th, 2020:
Wondering what's happening at Disney World tonight? Death is what's happening.
Wondering what's happening at Disney World tonight? Death is what's happening.


March 16th, 2020:
New information. ACE inhibitors increase expression of ACE2 and SARS-CoV-2 binds to ACE2. Those of us on antihypertensive ACE drugs may want to consider alternate hypertension medication.
https://www.thelancet.com/…/PIIS2213-2600(20)30116…/fulltext
Also French Government warning that ibuprofen and other anti-inflammatories should not be taken as they increase morbidity to COVID-19. Take acetaminophen (Tylenol) instead.
https://www.nytimes.com/…/14reuters-health-coronavirus-fran…
New information. ACE inhibitors increase expression of ACE2 and SARS-CoV-2 binds to ACE2. Those of us on antihypertensive ACE drugs may want to consider alternate hypertension medication.
https://www.thelancet.com/…/PIIS2213-2600(20)30116…/fulltext
Also French Government warning that ibuprofen and other anti-inflammatories should not be taken as they increase morbidity to COVID-19. Take acetaminophen (Tylenol) instead.
https://www.nytimes.com/…/14reuters-health-coronavirus-fran…
March 16th, 2020:
Italian Air Force. Single jet represents virus, meeting multiple jets streaming colors of Italian flag. Music in background is Pavoratti singing Pucchini’s “Nessun Dorma” (Let no one sleep). Lyrics contain “We shall overcome.”
https://www.youtube.com/watch?v=dwEfVIR27gY&feature=youtu.be&fbclid=IwAR3ljnejw8Hme2BII4akgj4OaKdoj4GCZcK7JhJeiU54nh03oQ4kFHUvCEU
Italian Air Force. Single jet represents virus, meeting multiple jets streaming colors of Italian flag. Music in background is Pavoratti singing Pucchini’s “Nessun Dorma” (Let no one sleep). Lyrics contain “We shall overcome.”
https://www.youtube.com/watch?v=dwEfVIR27gY&feature=youtu.be&fbclid=IwAR3ljnejw8Hme2BII4akgj4OaKdoj4GCZcK7JhJeiU54nh03oQ4kFHUvCEU
March 16th, 2020:
"The estimated median incubation period of COVID-19 was 5.1 days (CI, 4.5 to 5.8 days). We estimated that fewer than 2.5% of infected persons will display symptoms within 2.2 days (CI, 1.8 to 2.9 days) of exposure, whereas symptom onset will occur within 11.5 days (CI, 8.2 to 15.6 days) for 97.5% of infected persons. Horizontal bars represent the 95% CIs of the 2.5th, 50th, and 97.5th percentiles of the incubation period distribution. The estimate of the dispersion parameter is 1.52 (CI, 1.32 to 1.72). COVID-19 = coronavirus disease 2019."
Translation: On average people will show symptoms of COVID-19 within 6 days of infection. Within 12 days virtually anyone (97.5% of us) infected with the virus will show symptoms.
Day seven of lockdown for Finn and me @ Fluck Mill. Symptom free and trying to keep it that way.
https://annals.org/aim/fullarticle/2762808/incubation-period-coronavirus-disease-2019-covid-19-from-publicly-reported?fbclid=IwAR11dMu2xJlHRYnVhxMEDdkI6QD5XBUl3waNSbrzRb0--l1JFR4tqqBq0Ss
"The estimated median incubation period of COVID-19 was 5.1 days (CI, 4.5 to 5.8 days). We estimated that fewer than 2.5% of infected persons will display symptoms within 2.2 days (CI, 1.8 to 2.9 days) of exposure, whereas symptom onset will occur within 11.5 days (CI, 8.2 to 15.6 days) for 97.5% of infected persons. Horizontal bars represent the 95% CIs of the 2.5th, 50th, and 97.5th percentiles of the incubation period distribution. The estimate of the dispersion parameter is 1.52 (CI, 1.32 to 1.72). COVID-19 = coronavirus disease 2019."
Translation: On average people will show symptoms of COVID-19 within 6 days of infection. Within 12 days virtually anyone (97.5% of us) infected with the virus will show symptoms.
Day seven of lockdown for Finn and me @ Fluck Mill. Symptom free and trying to keep it that way.
https://annals.org/aim/fullarticle/2762808/incubation-period-coronavirus-disease-2019-covid-19-from-publicly-reported?fbclid=IwAR11dMu2xJlHRYnVhxMEDdkI6QD5XBUl3waNSbrzRb0--l1JFR4tqqBq0Ss
March 16th, 2020:
Findings from this article:
SARS-CoV-2 virus is transmitted by being encapsulated in water/snot (such as during a sneeze) and then being either aerosolized into the air (tiny droplets) or depositing on a surface.
In the air it can remain suspended up to three hours. In other words, if an infected person sneezes in a room it is possible for the air in the room to be contaminated for up to three hours afterwards. Air conditioning and heating ducting could carry the virus to other rooms in the building.
On a copper surface it can survive for up to four hours.
On cardboard (think Amazon box, your mail, napkins, etc.): 24 hours
On plastics (plastic bottles!) and stainless steel: 4 days
CAVEAT: This only speaks to survivability of the virus in the environment. There is no evidence yet that it can actually be transmitted by breathing contaminated air.
AND: The overwhelming method of transmission is direct human-human transmission via, well, spit. That means sneezing on your hands and giving someone a handshake. Or kissing (sorry, ladies), sharing food, etc.
Two studies in China seeking to understand why people who did not come in direct contact with each other in a given building nonetheless contracted COVID-19. Strongest evidence indicates that such infection occurs through common bathroom (restroom) facilities. Virus active on restroom door handles, sinks, toilets.
DISINFECTANT: The virus is wrapped in a "fat" cocoon. Therefore anything that dissolves fat is effective in killing it, including common soap. Surfaces that receive multiple human contacts (handrails, etc.) should be disinfected often but it makes no sense to constantly disinfect surfaces or objects that are only being touched by uninfected persons. So if you are hunkered down by yourself in your home, you don't need to disinfect your lightswitches constantly
CONCLUSION: The predominant method of transmission is direct human-human contact. Either by hands (i.e. handshake) or by having someone cough or sneeze on you.
https://www.nouvelobs.com/coronavirus-de-wuhan/20200314.OBS26035/combien-de-temps-le-coronavirus-survit-il-dans-l-air-et-sur-les-surfaces.html?fbclid=IwAR3wBsQ5xt3YbouJ-qW2Zx-RDfDXYFkUJlC0rd_EgWudGr4NkKVcj_KyjjE
Findings from this article:
SARS-CoV-2 virus is transmitted by being encapsulated in water/snot (such as during a sneeze) and then being either aerosolized into the air (tiny droplets) or depositing on a surface.
In the air it can remain suspended up to three hours. In other words, if an infected person sneezes in a room it is possible for the air in the room to be contaminated for up to three hours afterwards. Air conditioning and heating ducting could carry the virus to other rooms in the building.
On a copper surface it can survive for up to four hours.
On cardboard (think Amazon box, your mail, napkins, etc.): 24 hours
On plastics (plastic bottles!) and stainless steel: 4 days
CAVEAT: This only speaks to survivability of the virus in the environment. There is no evidence yet that it can actually be transmitted by breathing contaminated air.
AND: The overwhelming method of transmission is direct human-human transmission via, well, spit. That means sneezing on your hands and giving someone a handshake. Or kissing (sorry, ladies), sharing food, etc.
Two studies in China seeking to understand why people who did not come in direct contact with each other in a given building nonetheless contracted COVID-19. Strongest evidence indicates that such infection occurs through common bathroom (restroom) facilities. Virus active on restroom door handles, sinks, toilets.
DISINFECTANT: The virus is wrapped in a "fat" cocoon. Therefore anything that dissolves fat is effective in killing it, including common soap. Surfaces that receive multiple human contacts (handrails, etc.) should be disinfected often but it makes no sense to constantly disinfect surfaces or objects that are only being touched by uninfected persons. So if you are hunkered down by yourself in your home, you don't need to disinfect your lightswitches constantly
CONCLUSION: The predominant method of transmission is direct human-human contact. Either by hands (i.e. handshake) or by having someone cough or sneeze on you.
https://www.nouvelobs.com/coronavirus-de-wuhan/20200314.OBS26035/combien-de-temps-le-coronavirus-survit-il-dans-l-air-et-sur-les-surfaces.html?fbclid=IwAR3wBsQ5xt3YbouJ-qW2Zx-RDfDXYFkUJlC0rd_EgWudGr4NkKVcj_KyjjE
March 16th, 2020:
This is serious. I am calling on the Monroe County Health Department to officially diagnose COVID-19 cases by presentation of clinical symptoms, not laboratory tests. And to report all who prevent compelling clinical evidence of infection as officially infected to the state. We cannot afford to wait for the availability of laboratory testing nor can we rely on the federal government to make necessary resources, such as testing kits, to us in the numbers necessary.
The Health Department needs to do this to provide the political leadership with the information necessary to enable them to take appropriate action, today, to shut the city and county down. I.e. restaurant, bar, etc. closures.
Ashley Cranor, can you help?
This is serious. I am calling on the Monroe County Health Department to officially diagnose COVID-19 cases by presentation of clinical symptoms, not laboratory tests. And to report all who prevent compelling clinical evidence of infection as officially infected to the state. We cannot afford to wait for the availability of laboratory testing nor can we rely on the federal government to make necessary resources, such as testing kits, to us in the numbers necessary.
The Health Department needs to do this to provide the political leadership with the information necessary to enable them to take appropriate action, today, to shut the city and county down. I.e. restaurant, bar, etc. closures.
Ashley Cranor, can you help?
March 16th, 2020:
Stock market needs to announce that it will stop trading indefinitely until the administration puts someone like Dr. Fauci in directly charge of all messaging and action regarding coronavirus response. And that he is commander in chief of the armed force's response.
Stock market needs to announce that it will stop trading indefinitely until the administration puts someone like Dr. Fauci in directly charge of all messaging and action regarding coronavirus response. And that he is commander in chief of the armed force's response.
March 16th, 2020:
Talked to my doctor today about blood pressure medicine and ACE inhibitors. Article in Lancet (see below) indicates that ACE inhibitors, like the medication I take (Lotrel) can make COVID-19 worse.
His advice, through a nurse, was that he does not recommend going off them (I didn't want to go off, just switch to a different hypertension drug). I offered to email the Lancet article but they weren't interested, saying the science was essentially still up in the air.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30116-8/fulltext?fbclid=IwAR31induEV_9hRcaiSc8vwpvBvrURaVTgE55clI7DRPLO-o9Ozxsej-paIE
Talked to my doctor today about blood pressure medicine and ACE inhibitors. Article in Lancet (see below) indicates that ACE inhibitors, like the medication I take (Lotrel) can make COVID-19 worse.
His advice, through a nurse, was that he does not recommend going off them (I didn't want to go off, just switch to a different hypertension drug). I offered to email the Lancet article but they weren't interested, saying the science was essentially still up in the air.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30116-8/fulltext?fbclid=IwAR31induEV_9hRcaiSc8vwpvBvrURaVTgE55clI7DRPLO-o9Ozxsej-paIE
March 16th, 2020:
From my cousin, Elisabeth Sunday, who lives in France:
"Yup: We are headed towards mandatory nationwide quarantine. The president will speak at 8:00 pm, (in 10 minutes), and announce to all of France we have 48 hours to get where we want to be, then no one will be allowed out until further notice. We are expecting to be on total lockdown for anywhere from 8 to 12 weeks, possibly longer. Stay tuned! I'll comment after I've heard what he has to say."
From my cousin, Elisabeth Sunday, who lives in France:
"Yup: We are headed towards mandatory nationwide quarantine. The president will speak at 8:00 pm, (in 10 minutes), and announce to all of France we have 48 hours to get where we want to be, then no one will be allowed out until further notice. We are expecting to be on total lockdown for anywhere from 8 to 12 weeks, possibly longer. Stay tuned! I'll comment after I've heard what he has to say."
March 16th, 2020:
I've simplified my graphs somewhat. Hopefully they will be easier to understand.
There are two types of graphs. One shows the total number of infections for a given country. It also shows the death rate -- that is the % of people who die from the disease -- and the resolution rate -- that is the % of people who have either died OR recovered from the disease compared to the total number known infected.
What you want to see is a death rate as low as possible and a resolution rate (green line) as high as possible. A resolution rate close to 100% and a death rate close to 0% means the disease is essentially over in the given country. The first graph I will post here shows China, where that is true.
The second type of graph shows total infected, total dead and total resolved (dead or recovered) for a country. It also shows the rate of CHANGE in those numbers. On this chart what you want to see is the rate of change in deaths to be going down, the rate of change in infected to be going down. Rate of change in resolved is a little more tricky because you want more people to resolve via recovery and less people to resolve via death. So ignore it for now.
Again, use the China charts as examples of what you want all the charts to look like for a country that worked to get things under control. The Hong Kong charts are examples of what a country that didn't let things get out of control in the first place.
I've simplified my graphs somewhat. Hopefully they will be easier to understand.
There are two types of graphs. One shows the total number of infections for a given country. It also shows the death rate -- that is the % of people who die from the disease -- and the resolution rate -- that is the % of people who have either died OR recovered from the disease compared to the total number known infected.
What you want to see is a death rate as low as possible and a resolution rate (green line) as high as possible. A resolution rate close to 100% and a death rate close to 0% means the disease is essentially over in the given country. The first graph I will post here shows China, where that is true.
The second type of graph shows total infected, total dead and total resolved (dead or recovered) for a country. It also shows the rate of CHANGE in those numbers. On this chart what you want to see is the rate of change in deaths to be going down, the rate of change in infected to be going down. Rate of change in resolved is a little more tricky because you want more people to resolve via recovery and less people to resolve via death. So ignore it for now.
Again, use the China charts as examples of what you want all the charts to look like for a country that worked to get things under control. The Hong Kong charts are examples of what a country that didn't let things get out of control in the first place.
March 16th, 2020:
Man, there is a goddamn American hero on MSNBC right now. A woman, Jennifer Haller, is the first COVID-19 volunteer and just got herself injected with a potential vaccine.
She said "I am fortunate, I have a steady job a steady paycheck and my company is very supportive of this. My concern is those people who live paycheck to paycheck."
Man, there is a goddamn American hero on MSNBC right now. A woman, Jennifer Haller, is the first COVID-19 volunteer and just got herself injected with a potential vaccine.
She said "I am fortunate, I have a steady job a steady paycheck and my company is very supportive of this. My concern is those people who live paycheck to paycheck."
March 16th, 2020:
From my cousin, in France:
"Update from France: The entire country is on lockdown for a minimum of 15 days beginning at noon tomorrow, March 17. The lockdown can be prolonged if necessary. We must all stay in our homes and limit our time outside. Residents can not go out visiting, have visitors, hang out with friend in the park, or play games, or talk to anyone in person is not allowed. Boarders into and out of France are closed with some exceptions. We can only go to the nearest grocery store. All travel by car or by foot, must be authorized each time and each person must have a pass on their phones explaining our reasons for being out and why. There will be numerous checkpoints to check to see if your pass is in order. Even if you are jogging. you must have your pass or you will be fined. Everyone must limit their time outside. Shopping must be brief. We can also go to the doctor of course, or to work if that work is indispensable to keep the economy and country running. But most people are either working from home, or staying home because their businesses were closed. The state is reimbursing any loses and suspending payment on taxes and bills like electric, gas, and rent. Macron kept stating we are at war."
From my cousin, in France:
"Update from France: The entire country is on lockdown for a minimum of 15 days beginning at noon tomorrow, March 17. The lockdown can be prolonged if necessary. We must all stay in our homes and limit our time outside. Residents can not go out visiting, have visitors, hang out with friend in the park, or play games, or talk to anyone in person is not allowed. Boarders into and out of France are closed with some exceptions. We can only go to the nearest grocery store. All travel by car or by foot, must be authorized each time and each person must have a pass on their phones explaining our reasons for being out and why. There will be numerous checkpoints to check to see if your pass is in order. Even if you are jogging. you must have your pass or you will be fined. Everyone must limit their time outside. Shopping must be brief. We can also go to the doctor of course, or to work if that work is indispensable to keep the economy and country running. But most people are either working from home, or staying home because their businesses were closed. The state is reimbursing any loses and suspending payment on taxes and bills like electric, gas, and rent. Macron kept stating we are at war."
March 16th, 2020:
Three things the government needs to do:
1. Mobilize the military to build field hospitals, everywhere. Think M*A*S*H
2. Make it possible, easy even, for everyone, starting with the most at-risk, to stay at home. That means no taxes, no mortgages, no bills, no nothing. And $1000 a month in cash, per person in the household, to buy food and other necessities.
If you think that's going to be expensive, let me tell you about the alternatives.
Three things the government needs to do:
1. Mobilize the military to build field hospitals, everywhere. Think M*A*S*H
2. Make it possible, easy even, for everyone, starting with the most at-risk, to stay at home. That means no taxes, no mortgages, no bills, no nothing. And $1000 a month in cash, per person in the household, to buy food and other necessities.
If you think that's going to be expensive, let me tell you about the alternatives.
March 16th, 2020:
From the "mixed emotions" file:
"Scientists tracking the spread of the coronavirus reported on Monday that, for every confirmed case, there are most likely another five to 10 people in the community with undetected infections. These often-milder cases are, on average, about half as infectious as confirmed ones, but are responsible for nearly 80 percent of new cases, according to the report, which was based on data from China."
https://www.nytimes.com/2020/03/16/health/coronavirus-statistics-undetected.html
From the "mixed emotions" file:
"Scientists tracking the spread of the coronavirus reported on Monday that, for every confirmed case, there are most likely another five to 10 people in the community with undetected infections. These often-milder cases are, on average, about half as infectious as confirmed ones, but are responsible for nearly 80 percent of new cases, according to the report, which was based on data from China."
https://www.nytimes.com/2020/03/16/health/coronavirus-statistics-undetected.html
March 18th, 2020:
If you are worried about the reported spike in Italy's death rate, today, please consider:
Deaths occur 2-3 weeks after getting the disease. Italy's lockdown began 2 weeks ago. People dying today contracted the disease prior to the lockdown.
In a week or two we will start to see the effects of Italy's lockdown on the numbers.
If you are worried about the reported spike in Italy's death rate, today, please consider:
Deaths occur 2-3 weeks after getting the disease. Italy's lockdown began 2 weeks ago. People dying today contracted the disease prior to the lockdown.
In a week or two we will start to see the effects of Italy's lockdown on the numbers.